- See: Preparation for Proximal Tibial Cut:
- Discussion:
- intrameduallary & extrameduallary systems are available for aligning the proximal tibial cut;
- IM system is less accurate, particularly when tibia has varus bow and may lead to excessive cement column;
- ref: Extramedullary versus intramedullary tibial alignment guides for total knee arthroplasty.
- Application:
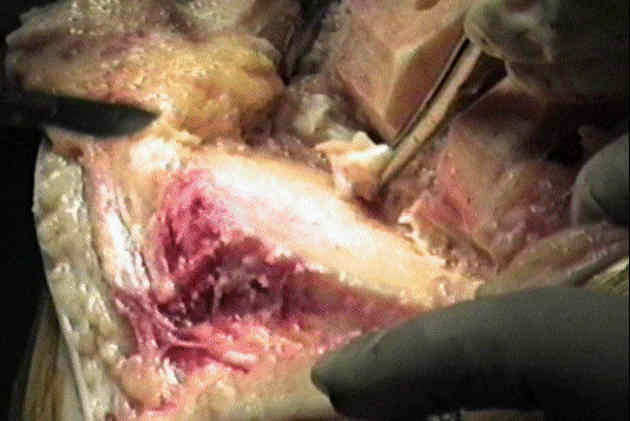
- knee is maximumly flexed w/ tibia distracted anteriorly & stabilized;
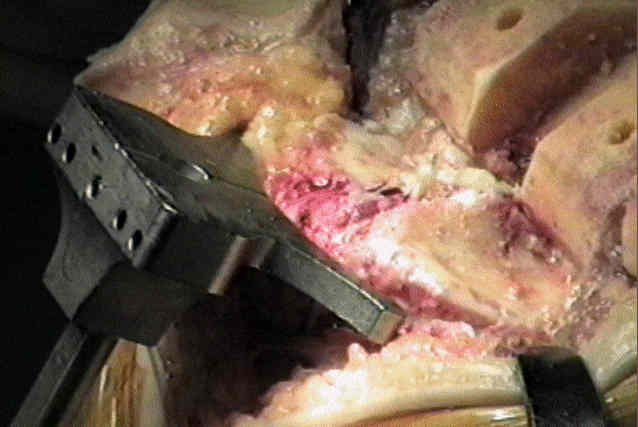
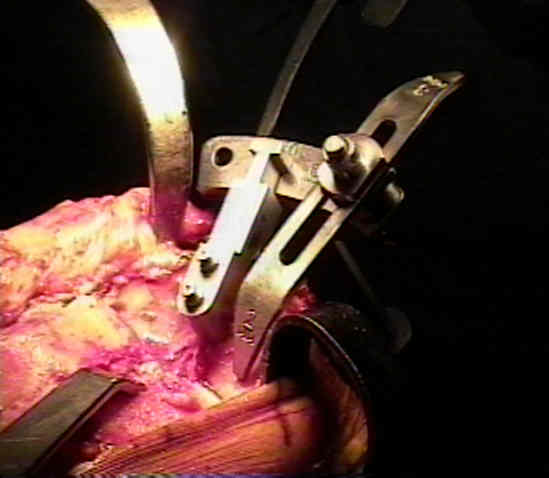
- proximal jig application:
- proximal guide is affixed in center of interspinous eminence of plateau;
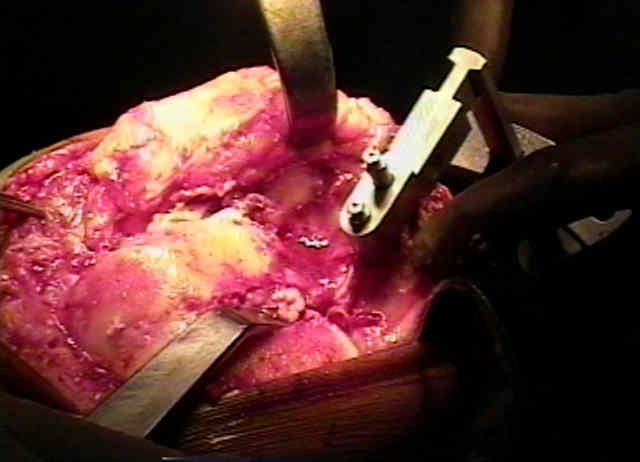
- proximal platform of tibial cutting guide conforms to the curved shape of the anterior cortex of the tibia;
- this allows the cutting platform to fit snugly up against the tibial cortex and improve the accuracy of the resection;
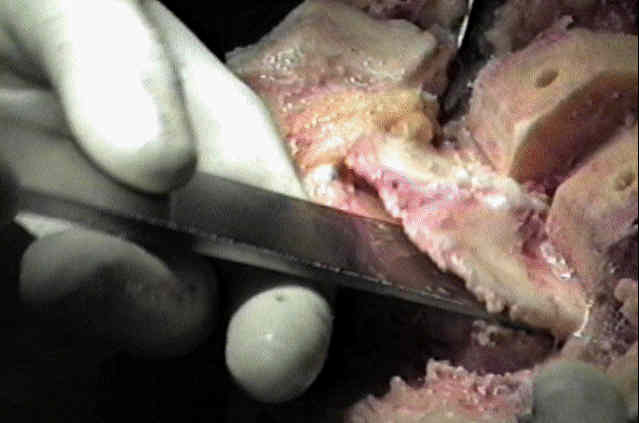
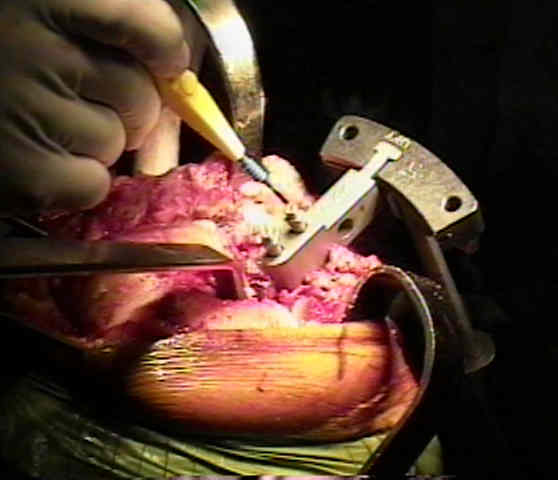
- depth of tibial cut
- tibial stylus is used to determine the exact level of resection;
- removable stylus protrudes from top of platform and telescopes up & down in 2 mm increments to help the surgeon
plan the level of resection;
- measurement off the lesser involved plateau:
- arms of platform are positioned against anterior tibial cortex at level 4-6 mm distal surface of less involved tibial cortex;
- upper platform is adjusted so stylus rests in center of condyle;
- measurement off the more involved plateau:
- if resecting to 0 deg on deficient plateau results in > 10 mm of resection from opposite plateau, deficient side should be
augmented w/ bone grafts or modular metal wedge;
- posterior slope
- both 0 deg and 5 deg cutting blocks are available in most systems;
- inaddition the cutting block assembly can be slanted posteriorly upto 5 deg, by moving the distal rod attachment anteriorly;
- Centering the Jig Assembly:
- because anatomic proximal tibia is generally in 3 deg of varus & because recommended resection angle is 0 deg, more bone is
typically taken from lateral condyle;
- centering the jig on the upper tibia:
- remember that jig systems fitted to anterior surface of proximal tibia will have a tendency to align in excessive internal rotation
because of everted patella tendon laterally;
- pass finger along the handle of the cutting guide, finger needs to brush against the medial edge of the tubercle;
- this places the axis of the component at the junction of the medial and middle thirds of the tubercle;
- avoid tendency to internal rotation, center the jig between the intercondylar tibial spines and center it on the medial 1/3 of the
tibial tubercle;
- An anteroposterior axis of the tibia for total knee arthroplasty.
- centering the jig on the tibial shaft:
- when properly oriented, guide is aligned w/ anatomic mechanical axis of tibia, and in most, it parallels anterior crest of tibia;
- tibial alignment rod is inserted into distal femoral cuttng guide, and the knee brought into full extension;
- references:
- Variability of extraarticular tibial rotation references for total knee arthroplasty.
- The anteroposterior axis of the tibia in total knee arthroplasty for chinese knees.
- The effect of rotational fixation error of the tibial cutting guide and the distance between the guide and the bone on the tibial osteotomy in total knee arthroplasty.
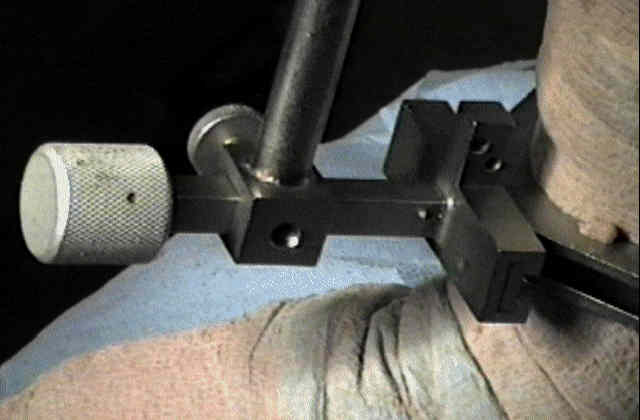
- centering the jig at the ankle:
- guides usually have centering device to localize distal portion of guide at center of ankle (point
slightly medial to intermalleolar axis;
- middle of tibia is approx 3-5 mm medial to the midpoint of ankle;
- mediolateral alignement is approx parallel to long axis of tibia, but as lateral mallelous is more
prominent, bisecting trans-malleolar axis will prejudice the cut slightly into varus;
- compensation is made by translating lower assembly medially so as to align it w/ center of
talus, which at transmalleolar plane, is at interval between EHL & EDL or palpable anterior crest of distal tibia;
- at the ankle, adjustments to alignment can be made in two planes:
- by sliding device away from the ankle, posterior slope can be applied to the tibial plateau resection;
- by sliding device medially & laterally at ankle, final adjustment can be made to centralize distal alignment over center of
talus & minimize chance for varus inclination of cut;
- references:
- The effect of ankle rotation on cutting of the tibia in total knee arthroplasty.
- Effects of tibial torsion on distal alignment of extramedullary instrumentation in total knee arthroplasty.
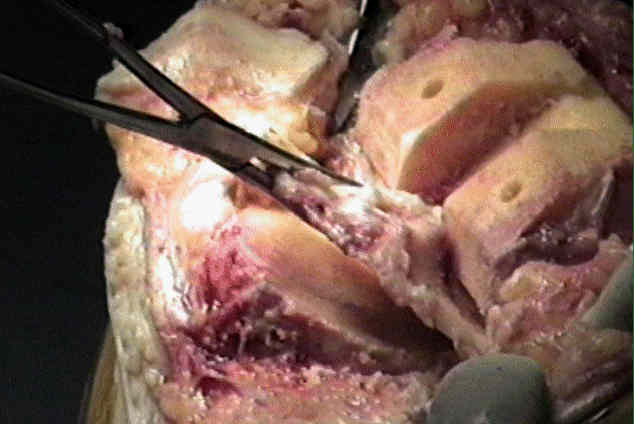
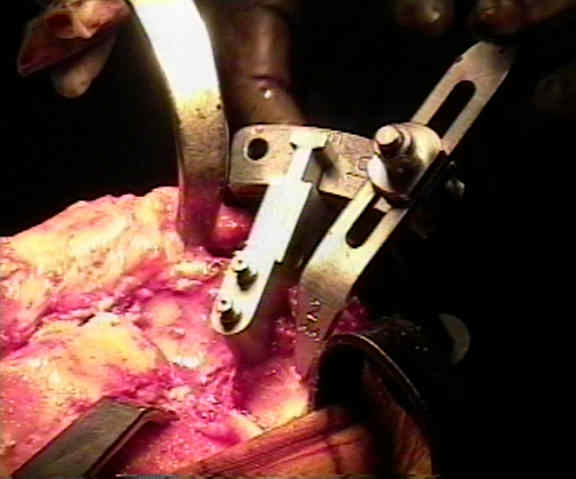
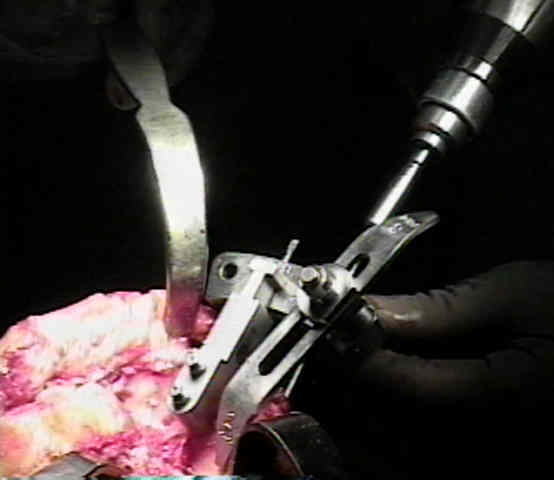
- Securing the Jig:
- a drill is inserted thru the proximal tibial cutting jig in preparation for insertion of fixation pegs;
- if fixation pins are inserted without prior drilling, then the pins will diverge instead of remaining parallell, which will prevent
subsequent adjustment of the cutting jig (if it is needed at the end of the case)
- Complications: Varus Positioning of Tibial Tray


Extramedullary versus intramedullary alignment guides in total knee arthroplasty.
- Johnson and Johnson