

- See: Tarsal Coalition
- Discussion:
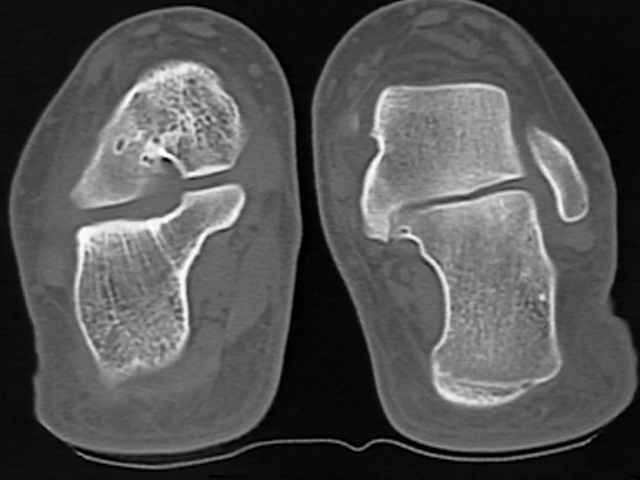
- talocalcaneal coalitions are characteristically on medial side of sub-talar joint;
- coalition tends to ossify between 12 and 15 years;
- although coalition between calcaneus & talus may occur in any of three facets, middle facet is most commonly involved;
- note that the anatomy of the middle & anterior facet may vary among individuals;
- four patterns are recognized;
- a single, small middle facet;
- a single middle facet that extends posteriorly and is almost as large as the posterior facet;
- middle facet that extends anteriorly
- two facets - middle & anterior facet- in medial compartment;
- classification of coalition:
- type I: osseous bridging of the middle facet joint;
- type II: cartilagenous coalition;
- type III: fibrous coalition;
- shows only slight narrowing of the middle facet joint;
- the coalition is located posterior to the sustentaculum tali (and in most cases standard CT scan protocols do not
image this area);
- these can be difficult to detect and may require bone scan to make the dx;
- Clinical Manifestations:
- talocalcaneal coalition generally becomes symptomatic in early teenage years when the preexisting cartilagenous coalition ossifies;
- patients often note repeated ankle sprains and may not be able to participate in sports;
- contraction and spasm of the peroneal muscles w/ forced inversion may be noted;
- subtalar motion is reduced;
- in few pts w/ large middle facet, tarsal tunnel syndrome develops from pressure on the median plantar nerve;
- large middle facet may also prevent full plantar flexion of the ankle, since it abuts the posterior portion of ankle joint;
- in these patients, resection will not improve subtalar motion;

- Radiographic Features
- CT Scan:
- can be used to make the diagnosis and can also be used to judge the relative size of the coalition;

- Non Operative Rx:
- conservative treatment is usually is usually effective in only 1/3 of patients with talocalcaneal coalition;
- use of below knee, wt bearing cast for 3-6 weeks may relieve symptoms;
- there after a plastizoate insert or an AFO is prescribed;
- symptoms often abate when facet ossifies completely, particularly if heel remains in a neutral position;
- Surgical Indications:
- results of talocalcaneal resections are less predictable than talonavicular;
- excision
- resection is treatment of choice in patients under 16 years of age if no degenerative changes are present;
- the middle facet coalition should be less than 50%;
- persistent hindfoot valgus may be assoc w/ poor result, & some recommend medial displacement os calcis osteotomy as an
adjunctive procedure;
- fusion:
- more than 50% involvement of middle facet or greater than 16 deg of valgus are relative contra-indication to resection;
- subtalar fusion is indicated when coalition is > 50% of middle facet or when degenerative changes in the tarsal joints exist (talar
beaking is not considered a degenerative change);
- failed resections are salvaged by subtalar fusion or triple arthrodesis;
- triple arthrodesis may be indicated when symptoms are severe and degenerative changes are present;
- Operative Treatment:
- incision starts medial to the talonavicular joint and extends to a point 1 cm distal to the medial malleolus;
- surgical approach for resection of talocalcaneal coalition is just anterior to the FHL;
- flexor hallucis longus lies just plantar to sustentaculum tali, & tendon can be used for orientation to the coalition anomaly;
- FHL tendon sheath is incised, and the tendon is retracted inferiorly;
- the sustentaculum tali and its associated coalition are identified;
- once coalition is resected, interposition of one half of the FHL tendon will decrease the chance of recurrence
Excision of symptomatic coalition of the middle facet of the talocalcaneal joint.
Treatment of symptomatic talocalcaneal coalition.
Resection for symptomatic talocalcaneal coalition.
Osseous and non-osseous coalition of the middle facet of the talocalcaneal joint.
Surgical Management of Symptomatic Talocalcaneal Coalitions by Resection of the Sustentaculum Tali.