

- See:
- Posterior Pelvic Injury:
- Sacroiliac Fracture Dislocations:
- Sacral Stress Fractures:
- Classification:
- zone I:
- frx across sacral ala can cause L5 nerve root impingement;
- about 6% of these patients will have neurological injuries;
- ref: Direct anterior decompression of L4 and L5 nerve root in sacral fractures using the pararectus approach: a technical note.
- zone II:
- frx thru neuroforamina can cause unilateral sacral anesthesia;
- frx involving the neural foramina require operative debridement of frx fragments prior to reduction and fixation
(through posterior approch);
- ref: Zone 2 sacral fractures managed with partially-threaded screws result in low risk of neurologic injury.
- zone III
- frx thru body of sacrum can cause highest incidence of injury to cauda equina and result in neurogenic bladder;
- about 56% of these patients will show neurological injuries
- ref: Functional outcomes of Denis zone III sacral fractures treated nonoperatively.
- misc:
- transverse fractures;
- U shaped fractures:
- results from axial loading;
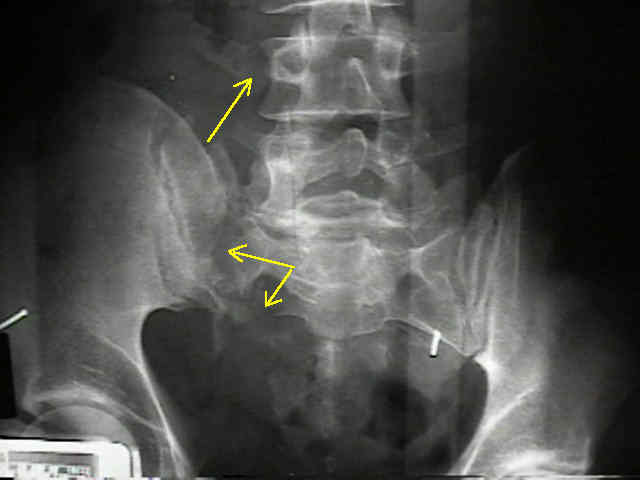
- radiographs:
- bilateral transforaminal sacral fractures and irregularities, L5 transverse process frx;
- paradoxic inlet view: on standard AP view, the upper sacrum appears as inlet view;
- ref: Percutaneous stabilization of U-shaped sacral fracture using iliosacral screws: technique and early results.
- Associated Injuries:
- if the sacral fracture is impacted w/ no verticle displacement, it may represent a LC fracture (therefore look for
anterior pelvic injury);
- w/ vertical displacement, the sacral frx may represent a Malgaine frx equivolent;
- Physical Exam:
- displacement in vertical plane is diagnosed by applying one hand to pelvic iliac crest and using other to apply traction to leg which
should cause displacement in vertical plane;
- Radiology: (see outlet view);
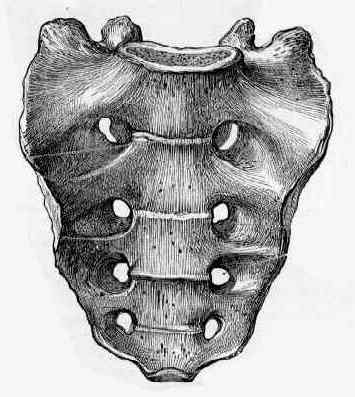
- sacral arcuate lines:
- will help delineate anatomy of frx of upper sacrum;
- sacral arcuate lines are composed of inferior surfaces of costal elements that form roofs of anterior sacral canals (foramina) &
neural grooves;
- arcuate lines are easily visible on AP view of pelvis & are symmetrical;
- asymmetry or discontinuity of sacral arcuate lines may be caused by uncomplicated sacral fracture ;
- disorganized or marked disruption of sacral arcuate lines is indicative of comminuted sacral fracture;


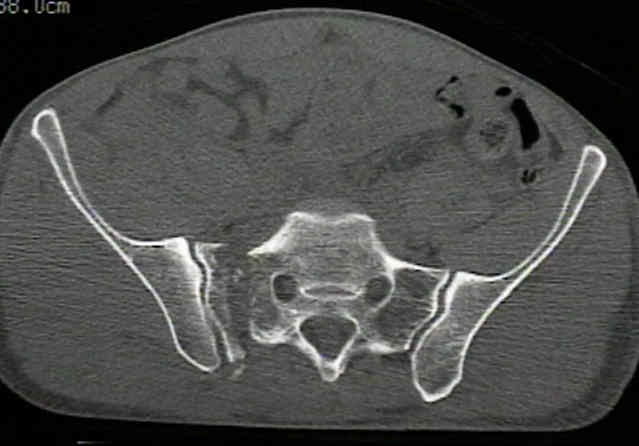
- CT scan: 
- Determine Frx Stability:
- stable fracture includes impacted vertical fracture of sacrum, nondisplaced fracture of posterior sacroiliac complex; or subtle
fracture of upper sacrum as seen by asymmetry of sacral arcuate lines;
- unstable frx, is characterized by frx diastasis of more than 0.5 to 1 cm, along w/ an unstable anterior injury;
- the other question, however, is the amount of healing potential;
- if a type I fracture reduces w/ traction, then the unstable frx would be expected to become sticky in about 4 weeks and would
expect complete healing in 3 months;
- references:
- OTA highlight paper predicting future displacement of nonoperatively managed lateral compression sacral fractures: can it be done?
- Nonoperative immediate weightbearing of minimally displaced lateral compression sacral fractures does not result in displacement.
- Conservative management of transverse fractures of the sacrum with neurological features. A report of four cases.
- Bilateral Sacral Ala Fractures Are Strongly Associated With Lumbopelvic Instability
- Surgical Approach to Fractures of the Sacrum:
- patient is in the prone position on a flouro table;
- similar surgical approach used for posterior approach to the SI joint
- posteror incision is made;
- additional vertical incision is made on opposite side;
- sacral nerve roots & frx site are visualized by placing laminar spreader at frx site or between the two superior ilac crests;
- decompression:
- decompression of sacral foramina (laminectomy) is helpful for patients w/ neurologic impingment;
- reduction:
- sacral frx reduction is usually achieved w/ pointed reduction forceps.
- forceps should span from spinous processes of sacrum to iliac crests;
- assess reduction by visualization of posterior sacral lamina & palpation of the fracture through the greater sciatic notch;
- sacral nerve roots are palpated after the reduction to be certain that they have not been entrapped;
- fixation:
- obtained w/ one or two screws into S1 vertebral body placed from lateral surface of the iliac wing; (similar to
SI joint dislocation);
- using flouroscopy, insert long 6.5 mm cannulated lag screws engage frx from the iliac wing to the body of S1;
- with transforaminal fractures, use fully threaded screw to avoid compression of the sacral neural foramina
- it may be possible to place a thin malleable plate placed across posterior sacrum from ilium to ilium as a tension band just
above greater sciatic notch;
- Sacroiliac Joint Fixation - Posterior screw fixation:
- it is important to note that malreduction of transforaminal sacral fractures will substantially decrease the space
available for iliosacral screws;
- surgeon should make all efforts to reduce transforminal fractures to within 1 cm of being anatomic;
- references:
- The effect of sacral malreduction on safe placement of iliosacral screws. Reilly et al. (15th Meeting of OTA 1999).
- Small bowel obstruction from entrapment in a sacral fracture stabilized with iliosacral screws: case report and review of the literature.
- The incidence of and factors affecting iliosacral screw loosening in pelvic ring injury.
- 4.5 mm reconstruction plate: (Albert, et al (1993));
- indicated for posterior pelvic fractures as well as sacral fractures;
- reconstruction plate is placed along dorsum of the sacral and through the posterior iliac spines (transiliac plate fixation);
- patient is placed in the prone position;
- two incisions are made over the PSIS which are perpendicular to the iliac wings, and one vertical incision is made over
base of the S1 spinous process;
- dissections are caarried down to the bony surfaces;
- predrill the PSIS to assist w/ reconstruction plate insertion;
- use the 4.5 drill to make 2-3 drill holes 1 cm lateral to the PSIS;
- an appropriately sized 4.5 mm reconstruction plate is chiseled thru the iliac spine, passed along the dorsum of the sacrum
to the opposite PSIS;
- recon plate is appropriately contoured;
- plate is fixed to the iliac wings using 6.5 mm cancellous screws, w/ two screws inserted into each ilac wing;
- reference:
- Posterior Pelvic Fixation Using a Transiliac 4.5 mm Recon Plate: a clinical and biomechanical study.
Sacral fractures: an important problem. Retrospective analysis of 236 cases.
Transverse fractures of the sacrum. A report of six cases.
Occult sacral fractures in osteopenic patients.
The effect of sacral fracture malreduction on the safe placement of iliosacral screws.
Surgical Anatomy of the Sacrum
Sacral Fractures: Current Strategies in Diagnosis and Management
Open Reduction Internal Fixation of Displaced Sacral Fractures: Technique and Results
Can Lumbopelvic Fixation Salvage Unstable Complex Sacral Fractures?