

- See: Acrosyndactyly;

- Discussion:
- failure of differentiation of the tisses between the fingers at 5th-8th week of intrauterine life (see limb development);
- most common in the middle and ring fingers;
- syndactyly (webbing or fusion of two or more digits), a result of failure of early interdigital tissue to degenerate;
- more common in white males, often is an autosomal dominant trait w/ incomplete penetrance;
- occurs in 2-3 per 10,000 live births;
- there is shortage of skin; combined circumference of two digits is 1.4 times the circumference of two digits held side to side;
- associated anomalies:
- classification:
- complete vs incomplete: (complete: entire length of digit is affected);
- synonychia: fingers share a common nail;
- simple vs complex:
- simple: skin only;
- complex:
- bony involvement;
- frequently there is also neurovascular involvement;
- when vessels are affected the bifurcation is more distal, and the branches are more rudimentary;
- syndactyly of the foot:
- great toe-2nd toe syndactyly may cause difficulty w. angular growth because of the relatively longer great toe, but this problem is uncommon and no
prophylactic treatment need be considered
- PreOp Planning:
- work up demands individual Allen's tests to each involved digit;
- radiographs to rule out tethering of digits;
- one side of digit should be operated on at a time, in order to avoid vascular insufficiency;
- w/ multiple syndactyly attention is first directed to border digits;
- vascular comprimise may occur if more than one digit is released at a time;
- usual stategy is to preserve as much regional skin as possible on the radial side of the involved digits (to maximize pinch sensation) and saving FTSG
for ulnar side of the affected digit;
- optimal age for release:
- traditionally, operation was postponed until age 3-4 years but currently many surgeons do release at age 9 months to 1 year;
- argument for delaying surgery is to avoid postoperative scarring, which may be more common in infants;
- w/ tethering of digits, patients may require even earlier release;
- in the case of syndactyly between ring and little finger, early flexion contracture w/ ulnar deviation may occur;
- with either thumb-index or ring little finger syndactyly, consider release at or before 6 months;
- bilateral procedures are done in children less than 14 months of age and avoided in the older child;
- surgical anatomy:
- cleeland's ligament:
- coalesce in interdigital space forming a dorsal roof over digital vessels and nerves as well as forming a septum between them;
- digital nerves and arteries may not be available for both digits;
- vessels may be entwined, or absent w/ in the bridge;
- aberent anatomy is more common w/ more complex deformities;
- nerves should be teased apart using magnification;
- Treatment: Simple Syndactyly
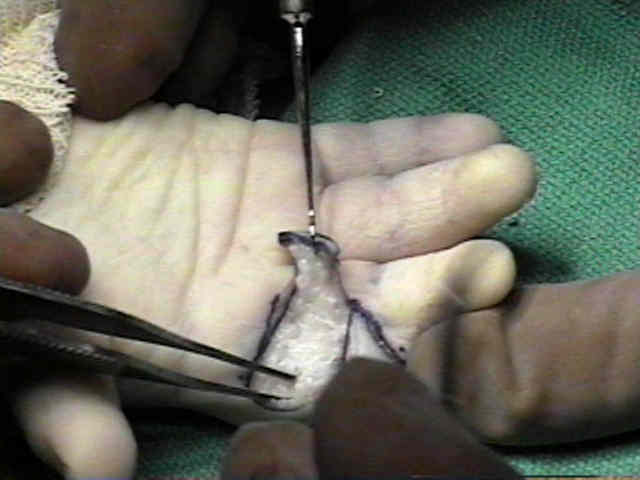
- positioning: consider applying stay sutures to the pulp of each digit to assist with retraction;
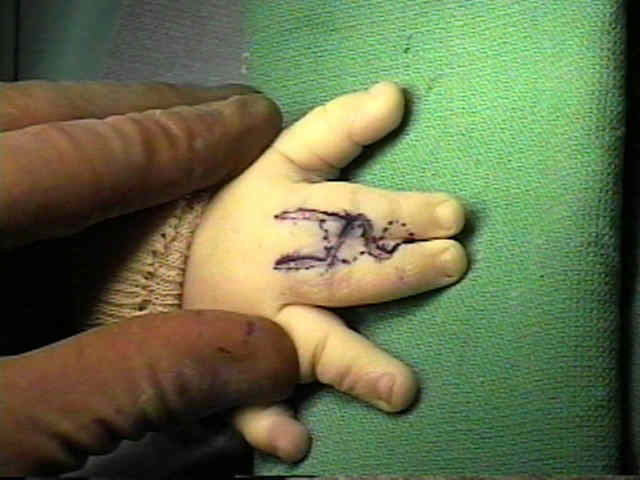
- mark skin flaps;
- consider inserting a 25 gauge needle thru syndactyly inorder to help plan interdigitating skin flaps on dorsal and plantar sides of fingers;
- web space:
- judge required depth of web space of reconstruction, based on appearance of web spaces of other digits;
- most commonly re-created using a proximally based dorsal flap, which extends from the MP joint up to level of the PIP joint (or just shy of it);
- wide web space is required to allow adequate spread of digits;
- it is essential that this flap be robust enough that a skin graft near the web space is avoided (because of the higher risk of "web creep";
- references:
- Syndactyly: can web creep be avoided?
- Long-Term Outcomes of Web Creep, Scar Quality, and Function After Simple Syndactyly Surgical Treatment
- dorsal flaps:
- the dorsal flap is raised as is described previously;
- triangular (zig-zag) flaps are raised with the base of the flap centered over the PIP and DIP joints of one finger;
- flap should extend to the mid-line of the adjacent finger;
- references:
- V-Y dorsal metacarpal flap: a new technique for the correction of syndactyly without skin graft.
- palmar flaps:
- make rectangular flap constructed to resurface one finger (typically other finger will require a full thickness skin flap);
- alternatively, make a flap that resembles an inverted T;
- zig-zag incision:
- then make triangular skin flaps which are designed to interdigitate with the dorsal skin flaps, by centering bases of the triangular flaps centered
over the PIP and DIP joints of the the opposite finger;
- palmar flaps begin at opposite corner to dorsal flap;
- reference:
- Syndactylism: results of zig-zag incision to prevent postoperative contracture.
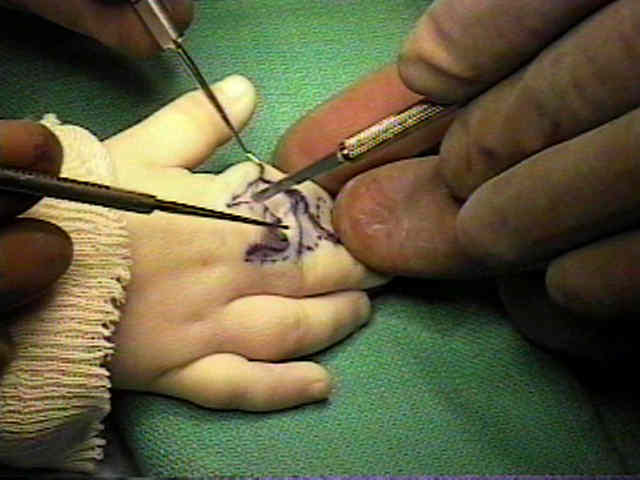
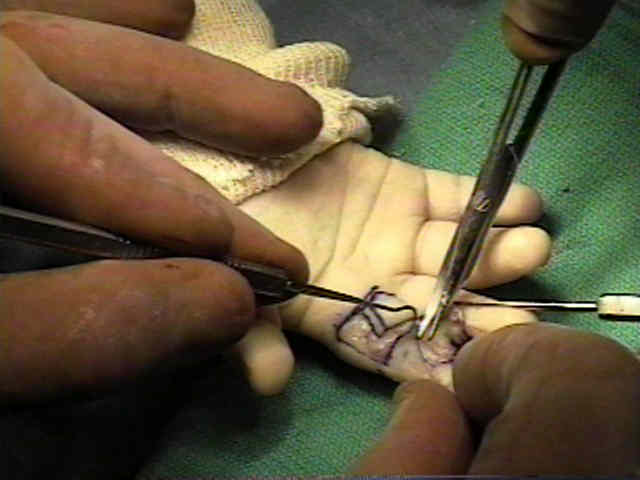
- digital separation:
- from the dorsal side, the interdigital connective tissue layer should be identified, befored attempting digital separation;
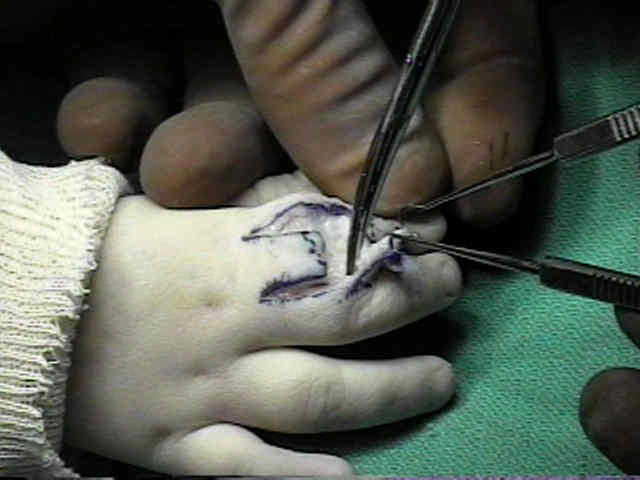
- digital separation should procede from distal to proximal, with the understanding that the digital artery bifurcation may be more distal than usual;
- manual spreading of the digits brings the soft tissue bridge under tension which facilitates the dissection;
- natatory ligament is incised;
- common digital artery division may limit the depth of the web dissection;
- in some cases, division of a proper digtal artery may be required;
- note that the limiting factor for the depth of the web is the division of the digital neurovascular bundle;
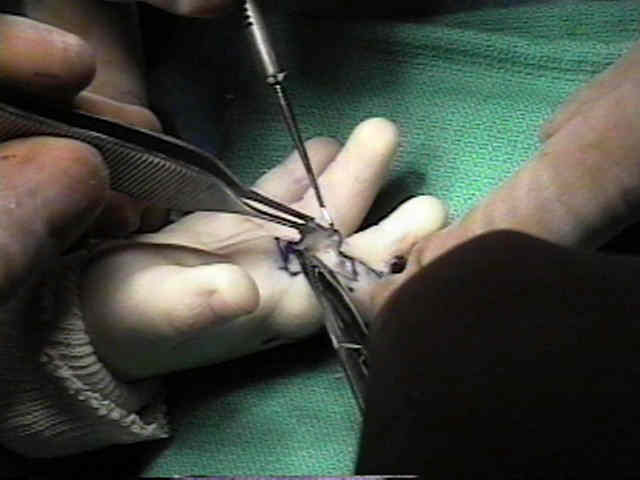
- defat the flaps:
- once digits are separated, both flaps are defatted;
- fat tissue is dissected along the neurovascular bundles along the entire digit and from the commissure;
- laterally fat tissue is removed as far as the middorsal line;
- in the report by Greuse M and Coessens BC (2001), the authors reported on 24 syndactylies without skin grafts in 16 consecutive patients;
- digital volume was decreased by defatting the full length of the fingers and the interdigital space. Closure of the zigzag incisions on both
fingers could then be achieved with minimal tension and did not seem to be related to the type of flap used for commissure resurfacing;
- they noted that defatting was a more important determinant of whether the wound could be closed without graft than flap configuration;
- reference:
- Congenital syndactyly: Defatting facilitates closure without skin graft
- full thickness skin graft:
- may be required, at the base of the digit next to the web;
- disadvantages include: hyperpigmentation, hair growth, donor site morbidity, scar contracture, and recurrence of the treated commissure;
- references:
- Full thickness grafts taken from the plantar instep for syndactyly release.
- Long-Term Outcomes of Web Creep, Scar Quality, and Function After Simple Syndactyly Surgical Treatment
- STSG:
- disadvantages include: hyperpigmentation, hair growth, donor site morbidity, scar contracture, and recurrence of the treated commissure;
- be aware that the skin of infants is much thinner than adults and therefore the dermaotome needs to be set on a thinner setting;
- in the report by Al-Qattan MM (2001), the author used split-thickness skin grafts when correcting Apert's syndactyly,
thinking that contraction of such grafts post-operatively would not cause any joint contracture or finger deviation;
- 8 patients whose average age at first surgery was 6 months;
- separation of all digits was accomplished before the age of 2 years;
- dorsal rectangular flap and interposing triangular digital flaps were utilised to create the web space and partially cover the skin defects in the fingers;
- remaining digital defects were covered with thin STSG which took fully in all cases;
- at final follow-up (1-6 years), the areas covered by skin grafts have reduced in size significantly because of skin graft contraction;
- this did not result joint contracture or digital deviation;
- references:
- The use of split thickness skin grafts in the correction of apert's syndactyly
- nail deformities:
- conjoined nails & underlying bone or cartilage needs to be freed;
- lateral nail folds may be recreated from two horizontal nail flaps on both side of fingers;
- palmar pulp is defatted and advanced dorsally to create a nail fold;





- Post Op Dressing:
- loss of skin graft and inadequate postoperative dressing;
- fingers should be abducted with a fluff stent, and held with a cling wrap and long arm plaster with the elbow flexed;
- Complications:
- web creep: progressive postoperative distal migration of the web
Ideas and Innovations: Surgical Method for Treatment of Syndactyly with Osseous Fusion of the Distal Phalanges.
Syndactylism: Results of zig-zag incision to prevent postoperative contracture.
Technical modification in repair of syndactylism.
Combined double Z plasty and Y-V advancement for thumb web contracture.
Evaluation of the operative treatment of syndactyly.
Syndactyly: can web space creep be avoided?
New modified method for the surgical treatment of syndactyly.
Evaluation of uniform operative technique to treat syndactyly.
The radiographic analysis of web height.
The Open Finger Technique for the Release of Syndactyly
Long-term results of syndactyly correction: Full-thickness versus split-thickness skin grafts