- Component Insertion:
- tibial insertion:
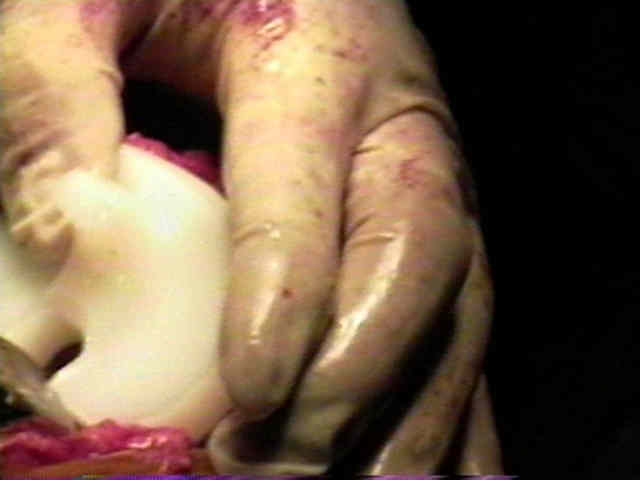
- cement is applied to the proximal tibial surface, and the surgeon uses gloved fingers to manually press cement into
proximal tibial surface;
- subsequently additional cement is applied to the proximal tibial surface;
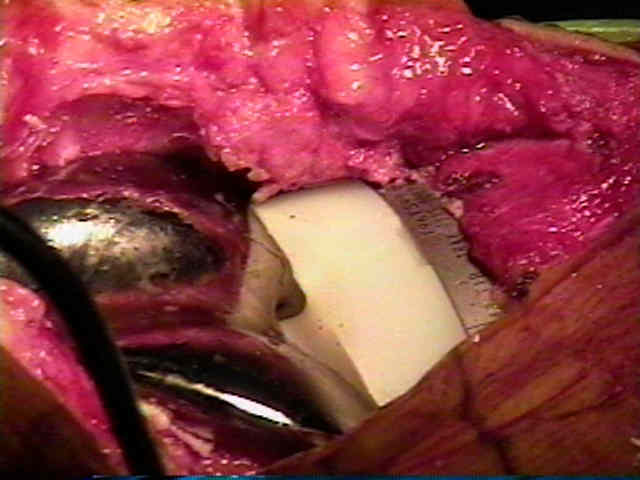
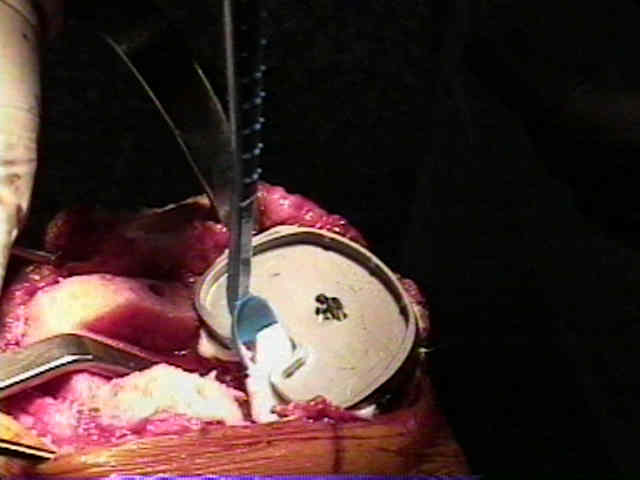
- tibial tray and its stem are precoated w/ cement and then are inserted;
- blocking lateral femoral condyle = appropriate rotational alignment
- note that external rotation of the femoral cuts & external rotation of the tibial component will complicate the insertion
of tibial component (lateral femoral condyle may block straight access for insertion of tibial component, which may
cause tibial component to rotate internally as it is inserted);
- this is prevented by levering a Homan retractor against the back of tibial plateau, which allows tibia to be subluxed
anteriorly and by hyperflexion of tibia;
- after impaction, & excess cement removal;
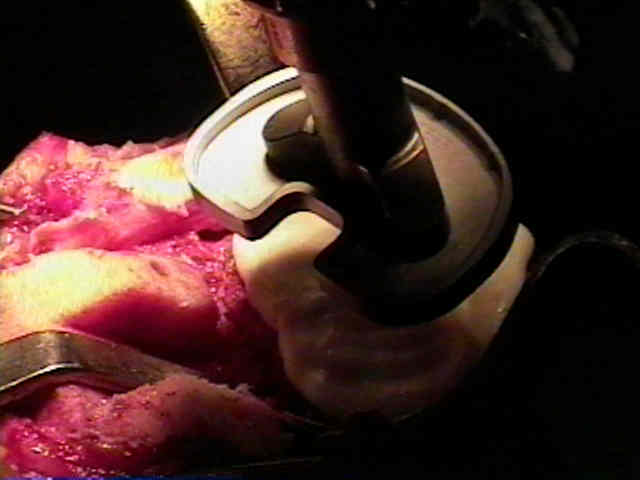
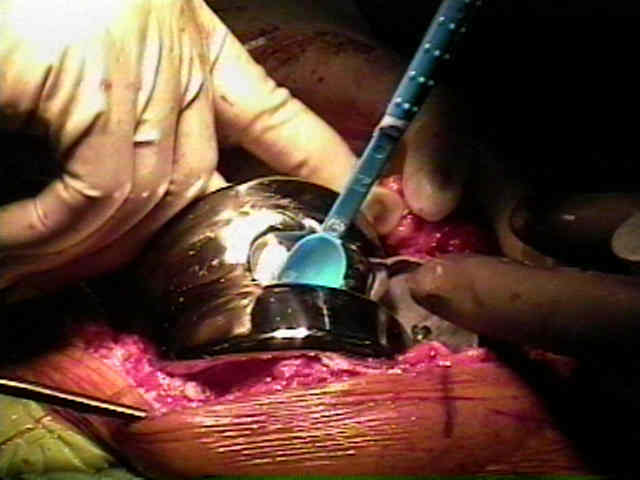
- femoral insertion:
- femoral component is then impacted into position and again, excess cement removed.
- take care to avoid femoral component flexion during the insertion (impact the femur in a slightly anterior direction);
- references:
- Cementing the femoral component in total knee arthroplasty: which technique is the best?
- Enhancing femoral cement fixation in total knee arthroplasty
- A different fixation of the femoral component in total knee arthroplasty may lead to preservation of femoral bone stock.
- plugging medullary canal:
- plugging of medullary canal may w/ bone graft may reduce blood loss but using cement to plug canal may a conduit for
biofilm formation;
- references:
- Plugging the intramedullary canal of the femur in total knee arthroplasty: reduction in postoperative blood loss.
- Sealing the intramedullary femoral canal with autologous bone plug in total knee arthroplasty.
- Sealing of intramedullar femoral canal in a TKA does not reduce postop blood loss: a randomized prospective study.


- trial component: trial spacer is placed;
- knee is then placed in full extension to further compress components while the cement hardens;
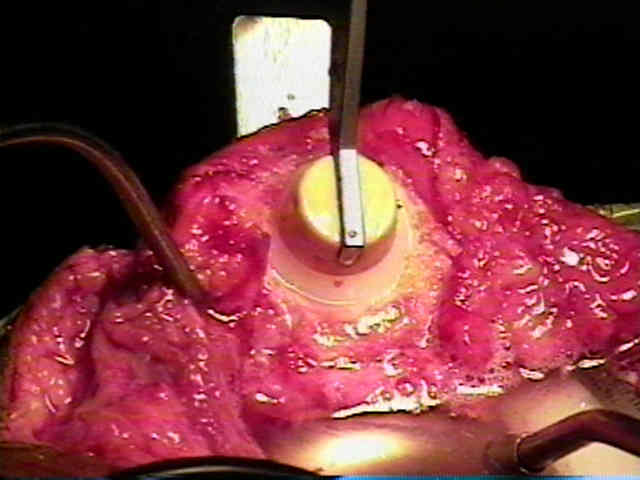
- patella is then cemented into position, using a patellar clamp to hold all-poly patellar component.
- cement fixation references:
- Reoperations after 3200 revision TKAs: rates, etiology, and lessons learned.
- Surgeon offers advice for optimal cement fixation in total knee arthroplasty: He notes that surgeons should consider cementing and pressurizing both the surface and tibial stem.
- Cement penetration with pulsed lavage versus syringe irrigation in total knee arthroplasty.
- The Effect of Cement Gun and Cement Syringe Use on the Tibial Cement Mantle in Total Knee Arthroplasty
- Final Testing of Stability and Tracking: (see instability post TKR)
- re-insert the trial polyethylene component and be sure that the patient is able to achieve full extension;
- it is certainly possible for both the femoral and tibial surfaces to rest on more than 1 mm of cement each, which could result in
incomplete flexion;
- if this is the case use a smaller polyethylene component;
- if lateral patellar subluxation is present, perform a lateral retinacular release;
- references:
- Influence of collateral ligament laxity on patient satisfaction after total knee arthroplasty: a comparative bilateral study
- Coronal laxity in extension in vivo after total knee arthroplasty
- The effect of anteroposterior laxity on the range of movement and knee function following a cruciate-retaining total knee replacement.
- Influence of anteroposterior and mediolateral instability on range of motion after total knee arthroplasty: an ultrasonographic study.
- Coronal plane stability before and after total knee arthroplasty
- A randomised controlled trial investigating the effect of posterior capsular stripping on knee flexion and range of motion in patients undergoing primary knee arthroplasty.
- Range of flexion after primary TKA: the effect of soft tissue release and implant design.
- Study shows stable knees post-TKA led to significant improvement in functional outcomes
- Collateral Ligament Laxity in Knees: What Is Normal?
- Intraoperative medial joint laxity in flexion decreases patient satisfaction after total knee arthroplasty.
- Cement Removal:
- after cement has hardened, excess cement is again removed w/ small osteotome and pickup;
- note that vigorous chipping of the excess cement can cause it to fly out and rebound off unsterile surfaces (such as OR lights
or the surgeon's face);
- replace the curved knee retractors and the Mchale retractor along the sides of the tibia to maximize exposure;
- remove any cement along the posterior surface of the tibia;
- clean the tibial tray of debris and soft tissue;
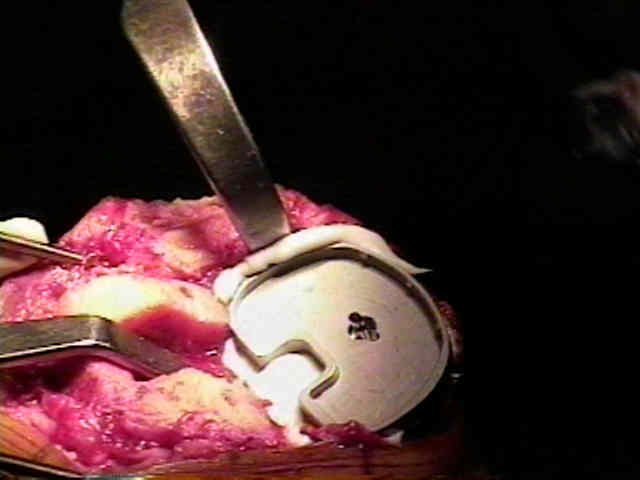
- Polyethylene Insertion:
- constraint options:
- some companies will offer constrained vs non constrained options;
- increased conformity increases the contact area and thereby reduces contact stress within the polyethylene
- increasing conformity also limits the ability of the femur to roll back during flexion, and may transfer increased shear stress
to implants (which could lead to increased loosening);
- curved knee retractors should be in place and the tibial subluxed forward;
- insert the definative polyethylene component, taking care that no soft tissue is entrapped by the polyethylene;
- this could cause incomplete seating of the component as well as pain from traction on the soft tissue