

 - Main Menu:
- Main Menu:
- PreOp Planning
- radiographs and templating
- Surgical Exposure:
- Patient Positioning, Preping, Draping
- Anterior Longitudinal Midline Approach
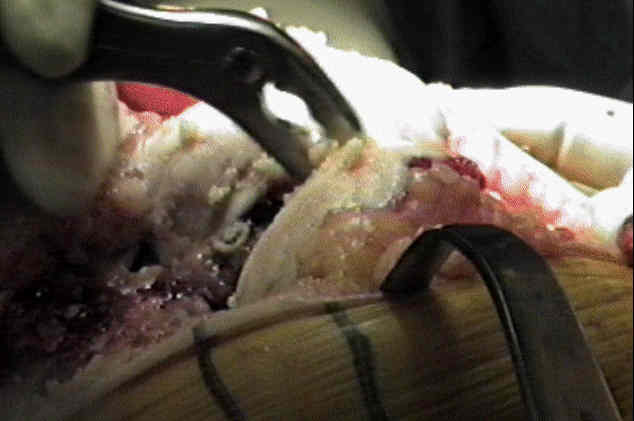
- Deep Articular Exposure
- Patellar Eversion:
- Patella:
- patellar resurfacing
- prior to patellar resurfacing, determine the propensity for the native patella to subluxate;
- if subluxation is present (tibial component is properly rotated), then patellar component should be medialized as much as possible;
- if patellar subluxation is present after patellar resurfacing, then perform a lateral retinacular release;
- patellar resurfacing can be performed early in the exposure in order to thin patella and facilitate eversion;
- non resurfaced patella considerations:
- patella baja (avoidance);
- Patella baja and total knee arthroplasty (TKA): etiology, diagnosis, and management
- Patellar impingement against the tibial component after total knee arthroplasty
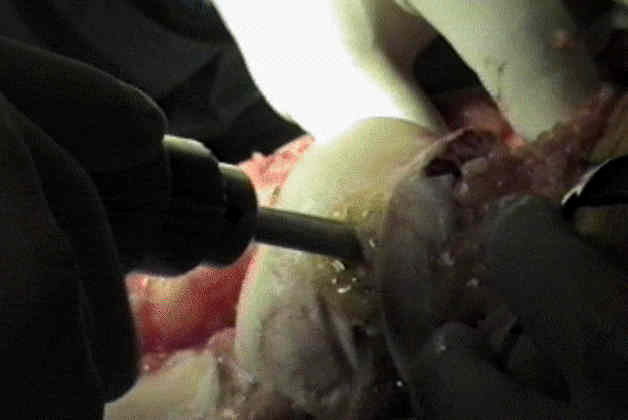
- Femoral Preparation:
- IM Alignment Rod
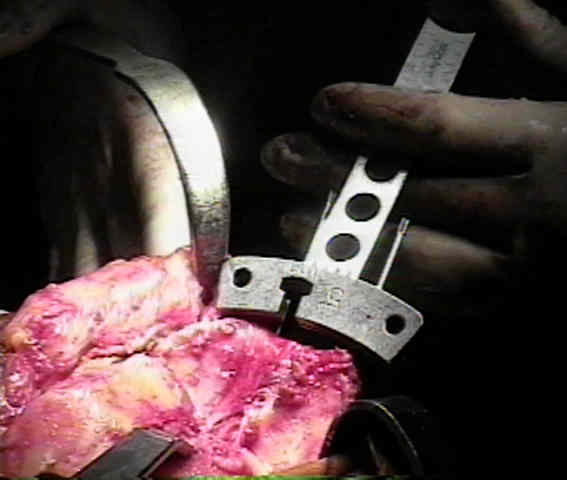
- Distal Femoral Resection: (avoid elevation of joint line)
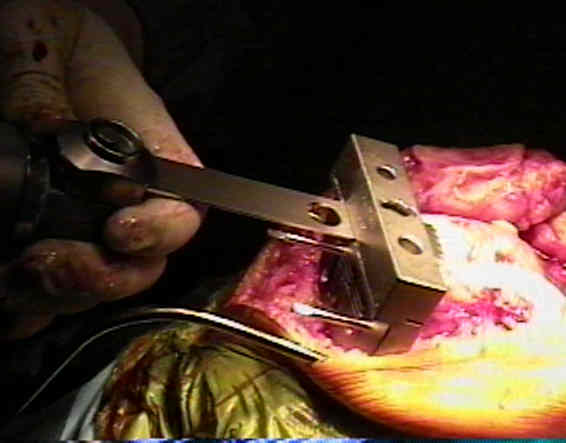
- Distal Femoral Sizing Guide: (rotational alignment)
- apply tibial extramedullary cutting guide to help align the femoral sizing
guide (should be a rectangle);
- Anterior, Posterior, & Chamfer Cuts:
- Box Cut: (for posterior stabilized prosthesis);

- references:
- Cutting errors in preparation of femoral components in total knee arthroplasty.
- Improved tibial cutting accuracy in knee arthroplasty.
- Excursion of oscillating saw blades in total knee arthroplasty.
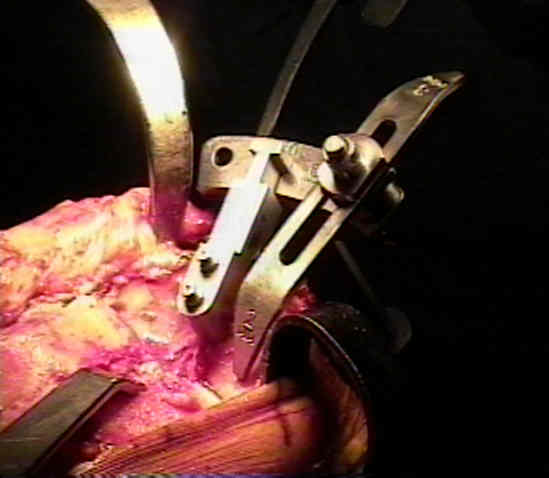
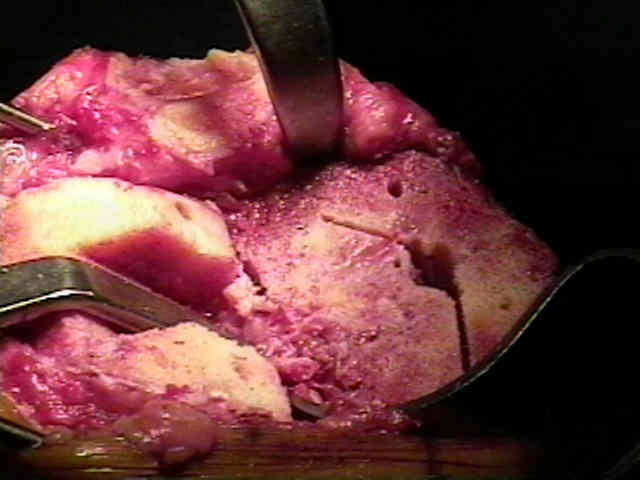
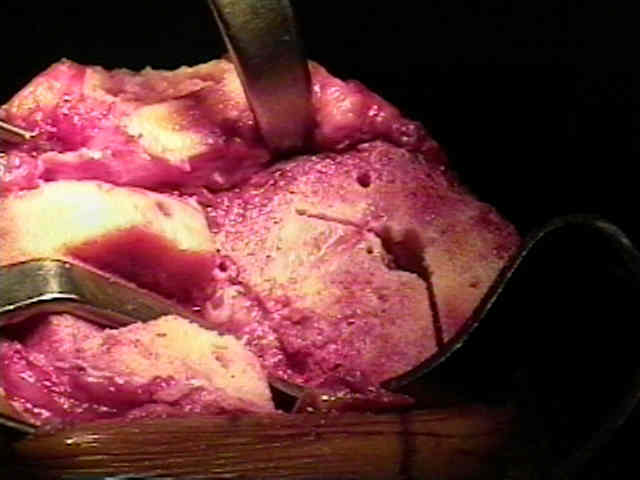
- Proximal Tibial Resection:
- preparation and exposure for the proximal tibial cut
- extramedullary guides
- rotation of tibial component
- posterior slope of the tibial component:
- depth of tibial cut (note joint line position)
- resect remnant menisci:
- it is important to sharply remove the remaining menisci, but beaware of the potential for vascular injury;
- popliteal artery lies behind the posterior horn of the lateral mensicus, and will be partially protected by the popliteus mucle;
- the popliteal vein lies directly posterior;
- menisci are removed by pulling them into the joint and transecting them w/ knife directed parallel to posterior tibial surface;


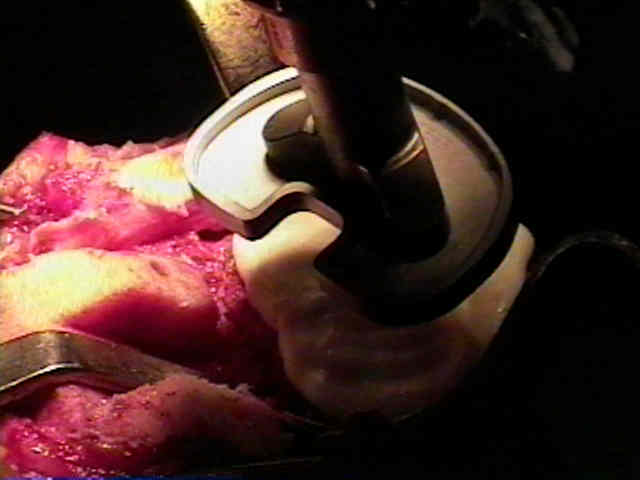
- Trial Components:
- Remove Posterior Osteophytes
- Sizing and Seating of the Tibial Tray
- rotation of tibial component
- bone grafts in TKR
- tibial stem
- test ROM, knee stability, and patellar tracking;
- it is wise to test patellar tracking before the patella is resurfaced;
- if subluxation is present, then the patella can be medialized;
- if subluxation is not present, then the patella can be placed in a central (or a slightly medialized) position;
- it is certainly possible to over-medialize the patellar component, which may cause the button to ride medially out of the notch;
- Tibial Stem Preparation:
- tibial trial plate is used as a jig to prepare seating holes for the pegs or stemm on the undersurface of the actual tibial component;
- be sure that rotation of tibial component is optimal;
- some jigs used to create canal for the tibial stem, will slightly wobble, meaning that the stem could inadvertently placed in varus;
- this is avoided by aiming the broaching devices towards the talus;

 - Cement Mixing:
- Cement Mixing:
- prior to cement mixing, be sure that:
- all of the components are on the table and have been placed in their respective inserters;
- ref: Femoral Bone Plug in Total Knee Replacement
- pulsatile lavage
- that the transected bony surfaces have been irrigated w/ pulsatile lavage;
- this will remove the fatty contents of the medullary canal, and will help to prevent fat embolization;
 - references:
- references:
- Pulsed lavage yields greater fixation strength in total knee arthroplasty
- Patellar component stability improves with pulsatile lavage in total knee arthroplasty.
- Component Insertion / Poly Insertion / Final Soft Tissue Release
- Wound Closure
- rush medical center betadine protocol:
- vancomycin powder, 1 gm, applied into knee cavity
- local anesthesia:
- Intraoperative Adductor Canal Block for Augmentation of Periarticular Injection in Total Knee Arthroplasty: A Cadaveric Study
- Efficacy of Intra-articular Local Anesthetics in Total Knee Arthroplasty
- local anesthetic administration: standford VA protocol:
- local Analgesia Infiltration Techniques – Hip and Knee Arthroplasty
- post operative dressing:
- reduction in bleeding:
- Postoperative Care:
- prevention of deep venous thrombosis
- evaluation of vascular injuries
- femoral nerve block
- physical therapy following TKR:
- ref: Impact of Psychological Distress on Pain and Function Following Knee Arthroplasty
- management of wound complications, hematoma, necrosis, and infection
- medical complications:
- management of postoperative fever:
- references:
- The Role of Blood Cultures in the Acute Evaluation of Postoperative Fever in Arthroplasty Patients
- Urinary-Bladder Management After Total Joint-Replacement Surgery.
- Pyrexia following total knee replacement.
- Febrile response after knee and hip arthroplasty.
- Fever: Fact and fiction.
- Evaluation of Postoperative Fever and Leukocytosis in Patients After Total Hip and Knee Arthroplasty
- Don't Do Unnecessary Work-ups for Elevated WBC After Lower-Extremity Joint Arthroplasty
- ileus:
- ref: Postoperative Ileus After Total Joint Arthroplasty
- adrenal failure/hemorrhage
- ref: Unilateral Adrenal Hemorrhage After Total Knee Arthroplasty