



- Discussion:
- diagnosis: limb is shortened, internally rotated, and adducted;
- Thompson and Epstein Classification:
- Type I: w/ or w/o a minor fracture
- Type II: w/ large single frx of post. acetabular rim;
- Type III: w/ comminution of rim of acetubulum w/ or w/o major frag;
- Type IV: w/ a fracture of the acetabular floor
- Type V: w/ a fracture of the femoral head;
- associated injuries:
- prior to closed reduction the surgeon must be aware of all associated injuries;

- Radiographic Evaluation of Hip Dislocation:
- AP of the Hip;
- pelvic series radiographs (AP, inlet and outlet);
- acetabular series radiographs (Judet views);
- radiograph of the femur and knee;
- Closed Reduction of Posterior Hip Dislocations:
- post reduction CT scan:
- look for concentric reduction and for the presence of intra-articular fragments or injury to the femoral head and/or acetabulum
- CT is esp useful with associated posterior wall fracture (to help predict stability);
- note high incidence of false negatives with CT (can miss intra-articular fragments);
- references:
- Reduction of posterior dislocation of the hip in the prone position.
- Irreducible fracture dislocation of the hip: a severe injury with a poor prognosis.
- Irreducible traumatic dislocations of the hip.
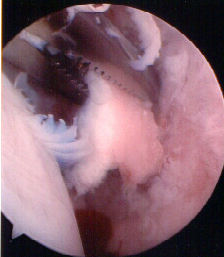
- Arthroscopic Removal of Loose Hip Joint Fragments:
- note that this technique is potentially dangerous due to the possibility that fluid may extravasate thru an associated acetabular frx, which would cause it to accumulate in the pelvis and abdomen;
- references:
- Hip arthroscopy for osteochondral loose body removal after a posterior hip dislocation
- Arthroscopy for hip dislocation and fracture-dislocation.
- Hip arthroscopy to remove loose bodies after traumatic dislocation
- Arthroscopic loose body removal after hip fracture dislocation: experiences in 7 cases
- Usefulness of arthroscopic surgery in hip trauma cases.

- Open Reduction of Posterior Dislocations
- Post-Reduction Radiographic Assesment:
- once closed reduction is obtained, carefully flex hip to 90 deg (if hip dislocates, it is unstable and reqires open reduction);
- radiographs:
- need to asses for congruency w/ repeat of pre-reduction radiographs;
- any widening of the joint space after reduction should suggest the possibility of loose fragments in the joint incomplete reduction of a fractured femoral head fragment, or soft tissue interposition;
- objective measurements include the distance from the femoral head to the ilioischial line compared to the contralateral hip;
- CT scan:
- always get post reduction CT scan to r/o iatrogenic posterior wall frx;
- 2 mm slices are required to help asses congruence;
- note the distance of anterior joint surface to femoral head as compared to the contralateral side;
- more than 0.5 mm difference is signifiant;
- small fragments which are located inferiorly, away from the wt bearing dome, do not necessarily need to be removed if the joint is congruent;
- post reduction 3 anatomical areas should be assessed;
- femoral head;
- femoral neck;
- acetabulum;
- Post Reduction Treatment of Stable Dislocation:
- avoid: flexion, internal rotation, and adduction;
- have abduction pillow present prior to closed reduction;
- traction is maintained until patient is pain free (1-2 wks)
- if needed, femoral traction pin may used for traction;
- Complications:
- Chondrolysis
- Degenerative Joint Disease:
- may occur in the majority of patients that sustain dislocation;
- Heterotopic Ossification
- may occur in the majority of patients with Pipkin III and IV frx;
- a relative contra-indication of XRT may be posterior hip dislocation w/ femoral head frx, since there is a theoretical risk of contributing to AVN or non-union;
- AVN after Hip Dislocation:
- incidence of AVN is 15% in posterior dislocation;
- incidence of AVN is approx 4% in anterior dislocation
Hip Dislocation: Current Treatment Regimens.
Computed tomography evaluation of stability in posterior fracture dislocation of the hip.
Reduction of posterior dislocation of the hip in the prone position.
Radiologic classification of posterior dislocations of the hip: refinements and pitfalls.
Plastic deformation and impaction of the retroacetabular surface associated with posterior fracture-dislocation of the hip: description of two cases..