

- See: Osteochondral Lesions of the Adult Knee
- Discussion:
- term OCD is a defect in the subchondral region with partial or compete separation of the bone fragment;
- most often seen on the postero-lateral aspect of the medial femoral condyle (about 80% of cases), and less often seen in posterior aspect of lateral condyle;
- is usually unilateral (74%)
- relatively common source of loss bodies in the knee or even an incongruous joint if the separated fragment is large;
- twice as common in males;
- classically occurs below the age of 18 (range: 6 to 53 years)
- etiology:
- repetitive overloading causing fragmention and separation of bony fragment;
- prognosis:
- depends on age at onset of symptoms & extent of involved wt bearing condyle;
- skeletally immature patients have better prgnosis and will frequently heal w/ non-op treatment if frag has not detached;
- lesions occurring after growth plate closure have worse prognosis are not likely to heal;
- bad prognosis if frag detaches, leaving defect in wt bearing region;
- classification: (from Clanton and DeLee (1982))
- I: depressed osteochondral fracture;
- II: osteochondral fragment attached by an osseous bridge;
- III: detached non-displaced fragment;
- IV: displaced fragment;
- Osteochondritis dissecans. History, pathophysiology and current treatment concepts.
- Clinical Manifestations and Exam:
- vague complaints: poorly localized pain, pain w/ exercise & effussion;
- loose bodies may cause locking;
- on exam, forcible compression of affected side of knee joint elicits crepitation during knee flexion and extension;
- in addition, affected femroal condyle is tender on palpation;
- w/ medial condylar lesion, pts may walk w/ the leg externally rotated inorder to avoid impingement of the lesion on the medial femoral condyle;
- forced range of motion of the internally rotated knee may cause pain;
- Radiographs:
- lateral view
- most lesions will lie between lines drawn along the posterior femoral condyle and along Blumensaats line;
- tunnel view;
- medial condylar defects may be better profiled w/ the knee in varying degrees of flexion;
- lesion may appear sclerotic;
- bone scan: bone scans can help defferentiate acute processes from chronic ones;
- MRI:
- findings usually correlate nicely w/ arthroscopic findings;
- may be used to determine whether the fragment is detached;
- Non Operative Rx in Skeletally Immature Patient:
- skeletally immature patients have better prognosis and will frequently heal w/ non-op treatment if frag has not detached;
- articular cartilage overlying these lesions should be normal & should protect the OCD defect during healing;
- fragment not separated:
- in the past, non-separated OCD lesions in patients < 12 years were treated w/ cast for 6 weeks;
- currently some recommend protected crutch walking and gentle ROM, since ROM is thought to have beneficial effects on cartilage healing;
- Operative Treatment:
- goal: maintainance of joint congruous & removal loose fragments;
- loose or detached fragment is removed with arthroscopy;
- small fragment: ( < 5 mm) or multiple OCD defects:
- fragments are removed & base of lesion should be drilled to create bleeding surface (better healing potential);
- large fragment ( > 5 mm) in wt bearing region:
- consider reduction and internal fixation;
- use standard Kirschner wires, resorbable Kirschner wires, AO, or Herbert screws.
- case example: kindly provdided by Dr. Lanny L. Johnson MD.


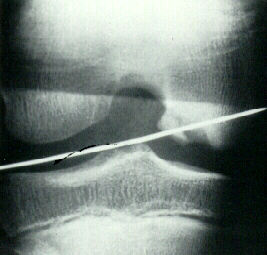
- K wire is followed by placement of cannulated lag screw, which is counter-sunk beneath the cartilagenous surface;;
- Lipscomb Method:
- partially detached lesions are reattached using K wires driven from within the knee joint and then driven out of the femoral cortex and the skin;
- the K wire is then pull proximally until the distal end is no longer visible from within the joint;
- the K wires are left subcutaneous in the distal thigh, and are removed after 6-8 weeks
Osteochondritis dissecans and osteochondral fragments managed by Herbert compression screw fixation.
Tibial cortical bone peg fixation in osteochondritis dissecans of the knee.
Osteochondritis dissecans of the patella. MRI evaluation and a case report.
Osteochondritis dissecans of the femoral condyles.
Compressive fixation of osteochondritis dissecans fragments with Herbert screws.
Osteochondritis disease in children.
Juvenile osteochondritis dissecans of the knee: etiology.
Osteochondritis dissecans of the knee. A long-term study.
Osteochondritis Dissecans of the Knee: Long-Term Results of Excision of the Fragment.
Outcomes of Osteochondral Lesions of the Knee Repaired With a Bioabsorbable Device