

- See: Humeral Frx - Main Menu 
- Condylar Fractures
- Non Union of Humeral Fractures
- Pediatric Humeral Shaft Fracture
- Synthes Humeral Shaft Products
- Discussion:
- mechanism:
- bending force produces transverse frx of the shaft;
- torsion force will result in a spiral fracture;
- combination of bending and torsion produce oblique frx w/ or w/o a butterfly fragment;
- compression forces will frx either proximal or distal ends of humerus;
- types of humeral shaft frx:
- transverse humeral fractures
- distal third frx
- short oblique fractures:
- displaced frx thru distal shaft are difficult to reduce & are difficult to maintain in reduced position;
- these fractures may be associated w/ delayed healing;
- long spiral fractures:
- spiral, comminuted, and oblique fractures have the advantage of generous fracture surface areas and tend to heal rapidly;
- if displaced with a gap which does not close when rotational alignment is restored, there may be muscle interposition;
- if left with good alignment, but with a significant gap between the frx frag, these frx go on to atrophic nonunion;
- associated fractures:
- A review of outcomes in 18 patients with floating elbow.
- Functional outcomes of "floating elbow" injuries in adult patients.
- Management of concomitant ipsilateral fractures of the humerus and forearm.
- Skeletal management of humeral shaft fractures associated with forearm fractures.
- Exam:
- need to rule out radial nerve palsy (see discussion), noting function of the ECRL/ECRB, EDC, ECU, EIP, and EPL;
- do not assume that every extension deficit reflects a radial nerve palsy (vs brachial plexus injury);
- references:
- Humeral shaft fracture with brachial artery injury.
- Management of fractures of the humerus in patients who have an injury of the ipsilateral brachial plexus.
- Acceptable Reduction: (forces displacing the fracture)
- axial malalignment:
- upper arm will accommodate 10-20 deg of anterior angulation & 10-30 deg of varus;
- this amount of angulation would be considered acceptable for patients w/ low to moderate functional demands;
- overriding fracture:
- bayonet position w/ upto 1 inch of shortening is acceptable;
- over-riding displacement is influenced to a degree by muscle contraction, which may have led to hanging cast principle;
- note displacing forces:
- frx just distal to insertion of deltoid muscle are prone to abduction of proximal fragment & also require special attention;
- Non Operative Treatment of Humeral Shaft Frx:
- note that these injuries are often very painful and that good initial immobilization is required;
- long arm splint needs to be applied from shoulder to wrist to fully immobilize the extremity;
- although rate of union is generally high with non operative treatment, incidence of mild malunion is high;
- in the study by Sarmiento A, et al (2000), the researchers were able to follow 620 patients with humeral shaft fractures that
were treated with cast bracing;
- 465 (75 %) of the fractures were closed, and 155 (25 percent) were open;
- non-union: 9 patients (6 %) who had an open frx vs 7 (less than 2 %) who had a closed fracture had a nonunion after bracing;
- 87 % of 565 patients for whom AP xrays were available, frx healed in less than 16 deg of varus angulation, and in
81 % of the 546 for whom lateral radiographs were available, it healed in less than 16 deg of anterior angulation;
- at the time of brace removal, 98 % of the patients had limitation of shoulder motion of 25 degrees or less;
- Functional bracing for the treatment of fractures of the humeral diaphysis.
- cast bracing:
- can be used for most closed humeral shaft frx;
- in most cases, cast braces are applied at 10-12 days following injury;
- forces displacing the fracture:
- hanging casts: may produce frx distraction & may increase risk of nonunion;
- reference:
- Tips of the trade #41. Modified coaptation splint for humeral shaft fractures.
- Outcome of nonoperative vs operative treatment of humeral shaft fractures: a retrospective study of 213 patients.
- Indications for Operative Treatment:
- unacceptable frx position following closed reduction;
- new onset radial nerve palsy following closed reduction;
- multi-trauma patients;
- open humeral fractures;
- segmental humeral fractures;
- floating elbow or ipsilateral arm injuries;
- pathologic fractures;
- references:
- Outcome of Nonoperative vs Operative Treatment of Humeral Shaft Fractures: A Retrospective Study of 213 Patients
- Acute Operative Management of Humeral Shaft Fractures: Analysis of the National Trauma Data Bank
- Operative Treatment:
- internal fixation should be reserved for fractures w/ inadequate reduction or patients with multiple trauma;
- IM Nailing of Humeral Shaft Fractures
- External Fixation of Humeral Frx
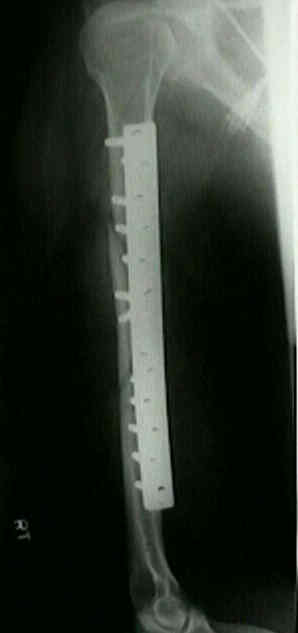
- Plate Fixation:
- anterior approach to humerus;
- posterior approach to humerus;
- Medial approach to treat humeral mid-shaft fractures: a retrospective study.
- Complications:
- Postoperative malrotation of humeral shaft fracture after plating compared with intramedullary nailing
Fractures of the shaft of the humerus. An epidemiological study of 401 fractures.
Traumatic segmental bone defects in the upper extremity. Treatment with exposed grafts of corticocancellous bone.
Reconstruction of the humerus with an intramedullary fibular graft. A clinical and biomechanical study.
Open reduction and internal fixation of humeral shaft fractures. Results using AO plating techniques.
Surgical treatment of humeral shaft fractures--the Basel experience.



 *
* 
