

- Discussion:
- prevalence:
- it represents approx 7% of all primary bone malignancies;
- second most common primary malignant bone tumor (behind osteosarcoma) (2.1 per 1 million children)
- Ewing's sarcoma is more common in males and is rare in blacks;
- source:
- uncertain origin;
- may arise from primitive reticulum cells of marrow;
- common karyotypic translocation between chromosomes 11 and 22;
- age:
- it is a tumor of children & young adults, w/ most cases occurring between ages of 10 and 20 years;
- 3% of Ewing's sarcoma occurs in children less than 3 years of age;
- 64% of Ewing's sarcoma occur in the second decade;
- genetics:
- expresses p30/32 MIC2 antigen (cell surface glycoprotein);
- 85% contain chromosomal translocation at the t(11;22)(q24;q12);
- prognosis:
- potentially the most lethal of all the bone tumors;
- most important adverse prognostic factor was metastatic disease detectable at the time of diagnosis;
- it almost always presents as a stage IIb lesion;
- before routine use of adjuvant chemo, pts w/ Ewing's were treated w/ XRT alone, & 5 year survival rate was no more than 15%;
- w/ use of adjuvant chemo, 5 year survival rate to more than 60%;
- w/ non metastatic Ewing's, disease free survival is 55-70% versus 22-33% for metastatic;
- pts require careful follow-up, due to post-XRT osteosarcoma;
- pelvic ewing's:
- tumors in pelvis are typically detected later & are therefore larger, with a poorer prognosis;
- 5 year survival rate is about 25%;
- differential diagnosis:
- osteomyelitis, osteolytic osteosarcoma, & EOG, & neuroblastoma;
- in infants and young children, rule out neuroblastoma (only 2% of patients with ewings sarcoma are less than 5 years of age);
- ewing's sarcoma will stain positve for PAS (cytoplasmic glycogen) and will have a positive vimentin stain;
- neuroblastoma stains negative for PAS and has a negative vimentin stain, but neuroblastoma is positive for neuron
-specific enolase and neurofilament;
- midshaft lesion w/ large, assoc soft-tissue swelling suggests either infection or Ewing's sarcoma;
- osteogenic sarcoma tends to be more metaphyseal;
- ref: Ewings sarcoma masquerading as osteomyelitis.
- Clinical Presentation:
- may mimic osteomyelitis w/ fever, elevated WBC, & sed rate, wt loss, anemia;
- enlarging, tender, bony prominence w/ an associated soft tissue mass;
- sites:
- femoral diaphysis > pelvis, tibia, humerus, fibula & ribs;
- develops in axial skeleton in large proportion of pts (about 40 %);
- tumors in pelvis are typically detected later & are therefore larger, with a poorer prognosis;
- lesion also has peculiar predilection for shaft of fibula
- an area containing little or no hematopoietic marrow;
- it occasionally arises in extraosseous sites ("soft-tissue, Ewing's").
- distant metastases are noted at diagnosis in about 20% of cases;
- Radiographs:


- permeative diaphyseal tumor w/ mottled, or patchy density;
- cortical involvement may produce periosteal reaction, "onion skin" pattern;
- references:
- Is PET Useful in Detecting Occult Nonpulmonary Metastases in Pediatric Bone Sarcomas?
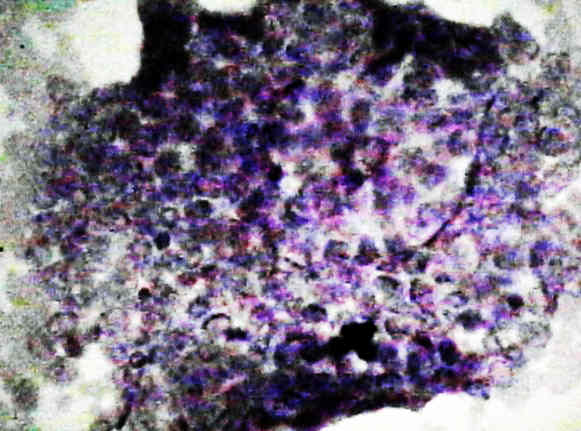
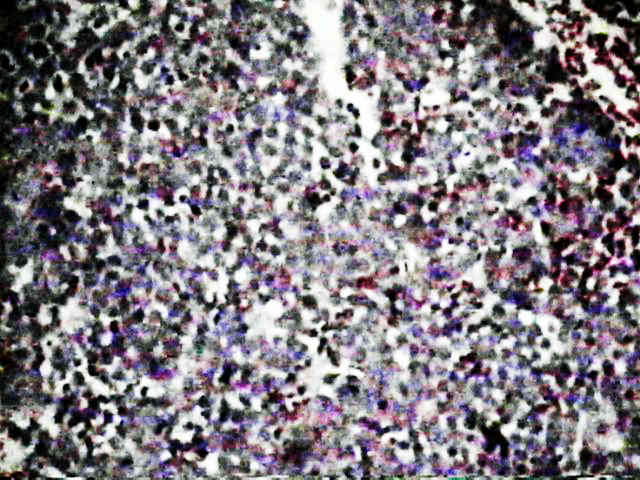
- Microscopic Features:
- Treatment:
- treatment consists of chemotherapy, surgical resection & possible XRT;
- w/ combined therapy pt survival has improved.
- reference: Outcomes and Prognostic Factors for Ewing-Family Tumors of the Extremities
- some authors recommend bone marrow aspiration and biopsy at two or more sites for staging purposes;
- radiotherapy:
- approx 75-85 % of primary ewing's tumors are sensitive, depending primarily on tumor size and site;
- poor to fair results are expect w/ large tumors located in axial skeleton;
- obviously XRT is not desirable in children because of its effect on the growing limb and because of the possibility for causing
secondary tumors (can be up to 20%);
- ref: Improved Prognosis for Patients with Ewing Sarcoma in the Sacrum Compared with the Innominate Bones: The Scandinavian Sarcoma Group Experience.
- chemotherapy:
- vincristine, doxorubicin, cyclophosphamide, adriamycin, ifosfamide, and etoposide;
- addition of chemotherapy with surgery increases survival to greater than 70% at 5 years;
- references:
- Ewing’s sarcoma. only patients with 100% of necrosis after chemotherapy should be classified as having a good response
- Tumor volume as a predictor of necrosis after chemotherapy in Ewing's sarcoma.
- wide surgical excision:
- preferred over XRT if:
- involved bone is expendable (eg fibula, rib, clavicle);
- if XRT would damage growth plate (XRT may cause premature closure of growth plate);
- if there is pathologic frx;
- limb salvage w/ insertion of long stem tibial component:



- References Local and systemic control in Ewing's sarcoma of the femur treated with chemotherapy, and locally by radiotherapy and/or surgery.
Is PET Useful in Detecting Occult Nonpulmonary Metastases in Pediatric Bone Sarcomas?