

- Considerations:
- anesthetic considerations:
- generally GEA is the standard of care:
- some anesthesiologists state that there is no such thing as safe pediatric conscious sedation;
- hematoma block may be dangerous and is usually ineffective;
- ensure that the neurologic examination is clearly documented on the chart;
- begin with gentle traction using finger traps, to determine the initial alignment of the ends of the radius and ulna;
- consider using the knee arthroscopy post, to assist with three point bending;
- w/ difficult reduction attempt to hook the distal ulnar fragment on the proximal fragment;
- subsequently procede to reduce the radial fragments;
- often the frx will have to be angulated in the direction of the original displacement (which relaxes the overlying intact periosteum) and then the distal fragment is pushed
out to length and then is hooked over the edge of the proximal fragment;
- for instance, w/ a distal both bones forearm frx, the distal radius is hyperextended and the distal fragment is pushed distally until the dorsal cortex is out to length;
- exaggeration of the deformity (often >90 degrees) should be performed to disengage the fragments;
- angulated distal fragment may then be apposed onto the end of the proximal fragment, with simultaneous correction of rotation
- the distal fragment is then "hinged over" the frx site;



- Acceptable Reduction:
- acceptable angulation is less than 15 deg, however, even more angulation may be preferable to restorting to open reduction;
- rotational alignment:
- difference in cortical widths of frx edges;
- relation of bicipital tuberosity to radial styloid;
- in full supination bicipital tuberosity should be prominent on ulnar side of radius;
- in neutral rotation the bicipital tuberosity should not be seen;
- difficult reduction:
- w/ difficult reduction consider muscle interposition at frx site;
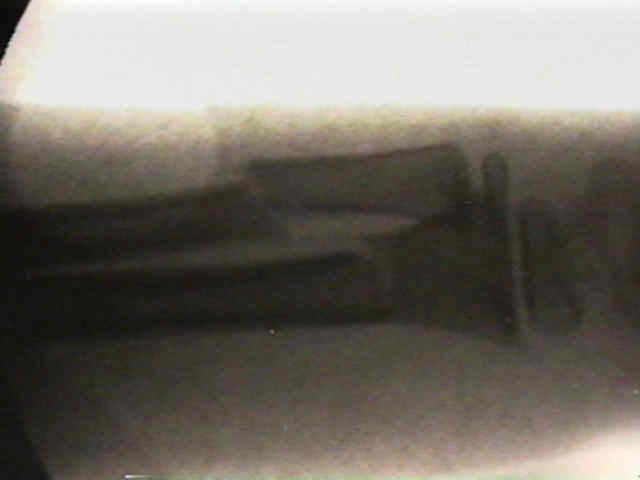
- reduction is verified under flouro by letting off traction & noting whether bone remains reduced or the fracture telescopes again;
- bayonet position is probably not longer acceptable; (historically was acceptable);
- if acceptable reduction cannot be obtained, then consider IM fixation with flexible titanium rods;
- position of immobilization is based on level of deformity; (deforming forces:)
- most proxial 1/3 frx need to be immobilized in slight supination;
- most middle 1/3 frx should be placed in neutral;
- most distal 1/3 frx require immobilization in slight pronation;
The effects of angular and rotational deformities of both bones of the forearm. An in vitro study.