- Preoperative Planning:



- Surgical Stratedgy:  - pt in true lateral position
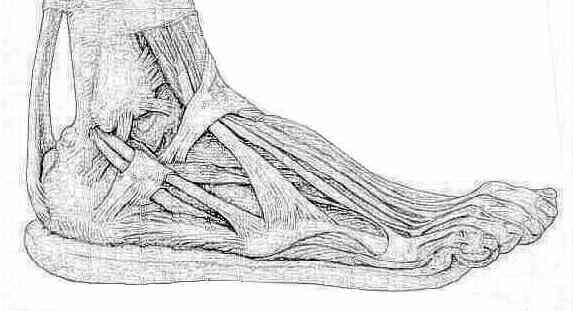
- J or L approach w/ subperiosteal dissection off lateral wall, including calcaneo-fibular ligament (sural nerve in flap);
- extension from tuberosity to calcaneo-cuboid (watch peroneals)
- reduction of critical angle of Gissane/ anterior process to sustentacular fragment;
- reduction of tuberostiy (height, length, and width of the heel);
- reduction of posterior facet;
- reduction of lateral wall;
- bone graft cancellous defects;
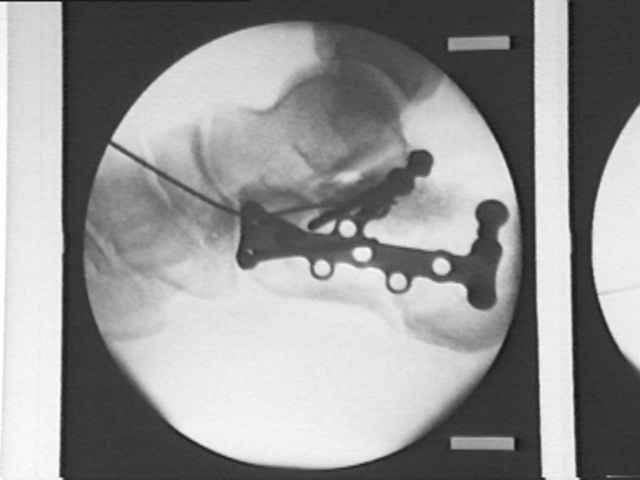
- plate fixation;
- early ROM, non wt bearing 10-12 weeks, hardware out = 1 year;
- pt in true lateral position
- J or L approach w/ subperiosteal dissection off lateral wall, including calcaneo-fibular ligament (sural nerve in flap);
- extension from tuberosity to calcaneo-cuboid (watch peroneals)
- reduction of critical angle of Gissane/ anterior process to sustentacular fragment;
- reduction of tuberostiy (height, length, and width of the heel);
- reduction of posterior facet;
- reduction of lateral wall;
- bone graft cancellous defects;
- plate fixation;
- early ROM, non wt bearing 10-12 weeks, hardware out = 1 year;
- Positioning and Preparation:
- patient is placed in true lateral position;
- ensure that all flouroscopic views including Broden's views and Harris heel view can be taken before prepping the patient;
- ensure that operative headlight is available;
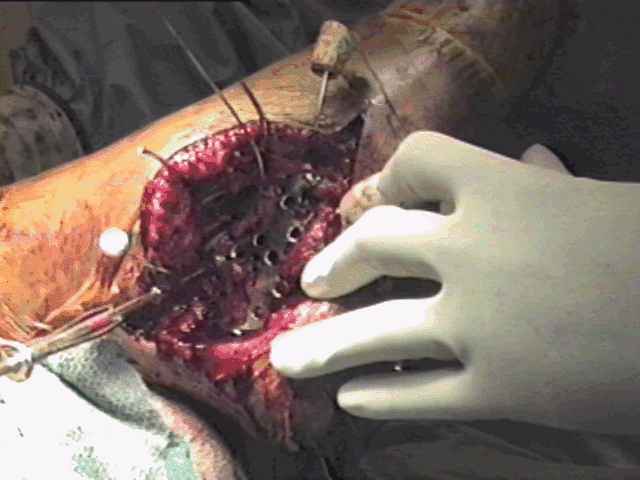
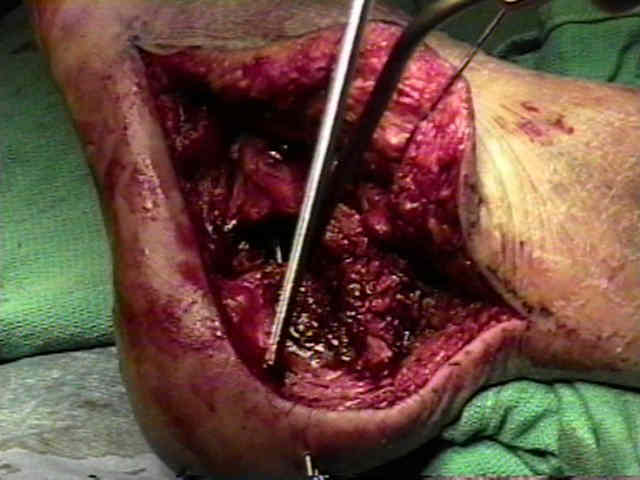
- Surgical Exposure: 
- Fracture Fixation:
- lateral wall is subperiosteally cleaned of soft tissue, & is gently pried laterally to expose the articular fracture fragments;
- restoration of height, width, and valgus position:
- large threaded Steinman pin is placed through the posterior superior portion of the calcaneal tuberosity;
- longitudinal traction is applied across the Steinman pin w/ a valgus vector applied as well;
- in some cases the anteromedial frx fragment (sustentacular frag) is displaced out of its normal position by the tuberosity fragment;
- disimpaction of the tuberosity fragment, will reduce the sustentacular fragment;
- anterolateral fragment:
- reduction of this fragment is necessary inorder to restore proper length;
- anterolateral fragment is reduced and fixed w/ a 3.5 mm cortical screw;
- alternatively, provisional fixation can be achieved w/ K wires which may need to be inserted thru the flap;
- tuberosity and sustentacular fragment reduction:
- restoration of heel width and height requires reduction of tuberosity fragment to the sustentacular fragment;
- generally the tuberosity fragment needs to be brought out of varus and a medially displaced position;
- articular reconstruction:
- note that the relationships between the sustentaculum and tuberosity fragments must be restored prior to articular reduction;
- malreduction of these fragments tends to crowd the space available for posterior facet reduction;
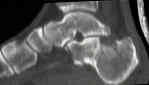
- posterior facet is evaluated;
- depressed fracture fragments are elevated "en mass" from the body of calcaneus;
- threaded Steinman pin is inserted through the posterior inferior corner of the calcaneus, across the posterior facet and into the talar body;
- this stabilizes the valgus reduction (i.e., fixation of medial wall corrects varus deformity);
- surgeon's finger is passed around the posterior facet in order to ensure that there is no step off between the tuberosity and the sustenaculum fragment;
- threaded Steinman pin is inserted through the posterior calcaneus into the cuboid;
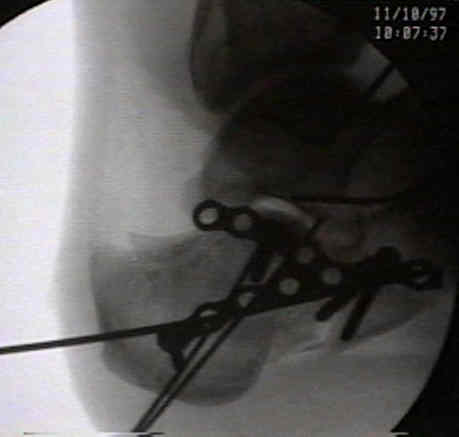
- plate fixation:
- bone grafting:
- see bone graft menu;
- in the presentation abstract by Buckley RE and Longino D, the authors determined whether or not autologous graft supplementation was beneficial in managing calcaneal fractures (Abstracts: OTA. JTO Vol 14 No 2. 2000)
- in the report by Schildauer TA, et al (2000), the authors used a synthetic injectable bone subsitute (Norian SRS) which allowed patients two weight bear as tolerated by 3 weeks postop; (see bone substitutes);
- Bone graft in the operative treatment of displaced intraarticular calcaneal fractures: is it helpful?
- Open reduction and augmentation of internal fixation with an injectable skeletal cement for the treatment of complex calcaneal fractures.






- Hazards:
- be aware that bicortical fixation of the medial fragment has a high risk of injurying the FHL, nerves, and vessels;
- wires placed in the subchondral bone of posterior facet or anteior to the critical angle of Gissane are at high risk for N/V injuries;
- in the report by Schildhauer TA, et al, infection rate was 11% (4/39 patients);
- smoking is a major risk factor, and patients should be told this prior to fracture;
- references:
- Open reduction and augmentation of internal fixation with an injectable skeletal cement for the treatment of complex calcaneal fractures.
- Internal Fixation of Calcaneus Fractures: An Anatomical Study of Structures at Risk.
- Post Op:
- regardless of type of treatment most authors recommend avoidance of wt bearing for 8 to 12 weeks following fracture;
- in the report by Schildhauer TA, et al, the authors noted that the application of Norian injectable cement (see bone graft substitutes), allow full wt bearing in some cases as early as 3 weeks;
- working person can often return to work at 4-6 months with an ankle brace;
- Open reduction and augmentation of internal fixation with an injectable skeletal cement for the treatment of complex calcaneal fractures.
- Controversies:
- supplemental external fixation:
- Open reduction and circular external fixation of intraarticular calcaneal fractures.
- Two-stage operative treatment of comminuted os calcis fractures. Primary indirect reduction with medial external fixation and delayed lateral plate fixation.
Intra-articular Calcaneus Fractures: A biomechanical comparison of two fixation methods
Surgical management of calcaneal fractures using bilateral incisions and minimal internal fixation.
Surgical management of fractures of the os calcis.
Operative treatment of intra-articular fractures of the calcaneus.
Fractures of the calcaneum: the anterolateral fragment.
Operative treatment in 120 displaced intraarticular calcaneal fractures. Results using a prognostic computed tomography scan classification.
Operative treatment of displaced intra-articular fractures of the calcaneum. Medium-term results.
Treatment of displaced intra-articular fractures of the calcaneus using medial and lateral approaches, internal fixation, and early motion.
Intra-articular fractures of the calcaneum. Part II: Open reduction and internal fixation by the extended lateral transcalcaneal approach.
Osteosynthesis of displaced intraarticular fractures of the calcaneus. Results in 123 cases.
Surgical treatment of displaced intraarticular fractures of the calcaneus. A combined lateral and medial approach.
Open treatment of acute calcaneal fractures.
The operative treatment of intraarticular calcaneal fractures. Indications, technique, and results in 257 cases.
Combined percutaneous and "minimal" internal fixation for displaced articular fractures of the calcaneus.
Extensive intraarticular fractures of the foot. Surgical management of calcaneal fractures.
Internal fixation of experimental intra-articular calcaneal fractures: A biomechanical analysis of two fixation methods.
Operative treatment of intra-articular fractures of the os calcis - the role of rigid internal fixation and primary bone grafting: preliminary results.