


- Distal Radial Length:
- shortening results from extensive comminution and impaction of frx fragments into the metaphysis;
- shortening of radius is more disabling than an angulatory deformity of the distal radius (ie, dorsal tilt or loss or radial inclination);
- radial shortening following distal radial frx may lead to acquired positive ulnar variance, ulnar impaction syndrome, and instability;
- patients will often have significant loss of pronation and suprination;
- some authors, in fact, note that radial shortening is only important in so much that it reflects a change in ulnar variance;
- usually a change of more than 3 mm of ulnar variance will lead to symptoms;
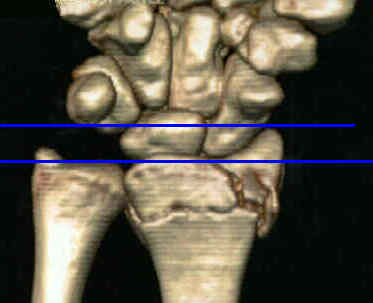
- radiographic measurement:
- for precise measurement, a true lateral radiograph of both wrists should be obtained in order to compare the radial lengths of the injured and the non injured wrists;
- mark two lines perpendicular to long axis of the radius;
- first line intersects tip of radial styloid;
- second line intersects distal articular surface of ulnar head;
- distance between two lines, is called radial length should be 11 to 12 mm;
- acceptable reduction:
- normal length of radius averages 9-12 mm;
- shortening of upto 3-5 mm can be associated w/ a satisfactory result, as long as there is an accurate articular restoration, however, the surgeon should strive to achieve less than 2 mm of shortening;
- greater than 10 mm of shortening is often associated w/ symptoms, including involvement of distal RU joint
- management:
- when radial shortening is due to comminution, then external fixation is the most reliable method of restoring length
Correction of Post-Traumatic Wrist Deformity in Adults by Osteotomy, Bone Grafting, and Internal Fixation.
Classification of distal radius fractures.
Fractures of the distal end of the radius in young adults: a 30-year follow-up.
Minor axial shortening of the radius affects outcome of Colles' fracture treatment.
Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation.