

see also (Radial Nerve Discussion; Tendon Transfers for Radial Nerve Palsy)
Discussion
- up to 18% of humeral shaft frx have an associated radial nerve palsy;
- it occurs most commonly with middle third humeral fractures & in Holstein Lewis fractures;
- types of nerve lesions;
- laceration of nerve, most common in spiral frx of the distal 1/3 of humerus;
- entrapment of radial nerve at fracture site by bone fragments;
- most often, palsy is a result of neuropraxia & are incomplete;
- w/ neuropraxia, nerve axons will regenerate 1 mm a day;
Palsy Associatted w/ Distal Third Frx
- radial nerve may be injured by fractures is at junction of mid and distal thirds of humeral shaft, esp if there is lateral displacement of distal fragment;
- at this location the radial nerve emerges from spiral groove & is tethered as it pierces the intermuscular septum;
- here, it cannot yeild to lateral displacement of distal fragment and therefore may be subject to neuropraxia;
Prognosis and Treatment
- w/ closed humeral frx, radial nerve f(x) will return by 3-4 months in 75%-90% of patients;
- most of these injuries represent a neuropraxia or axonotmensis;
- if nerve function does not return w/ in 3-4 months, then nerve should be surgically explored;
- exam should focus on the ECRL which will be among the first muscles to recover (wrist will extend in radial deviation due to weakness of ECU, which is innervated further distally by the PIN);
- negative prognostic findings:
- open humeral shaft frxs:
- incidence of radial nerve laceration is about 60%, hence, radial nerve should be explore primarily;
- nerve laceration (complete or partial);
- nerve entrapment in callus;
- Holstein Lewis fractures;
- open humeral shaft frxs:
- if nerve function disappears w/ fracture reduction, it means that nerve is caught in the fracture;
- hence, immediate exploration is required, to prevent further nerve damage, and/or entrapment of nerve by fracture callus;
Surgical Treatment
- consider preoperative EMG;
- if EMG shows at least some signs of recovery at 3 months, then consider waiting 1 month and repeating EMG to look for signs of further recover;
- note that EMG studies cannot distinguish from a severed nerve from an unrecovered intact nerve and does not detect recovery much earlier than a careful physical exam;
- high energy open fractures:
- nerve repair;
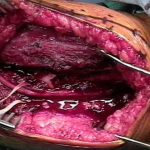
Case Example
- 13 year old male was casted for a distal humeral fracture but was left in significant varus. Radial nerve function was present in the ER but was not present one week later in clinic.
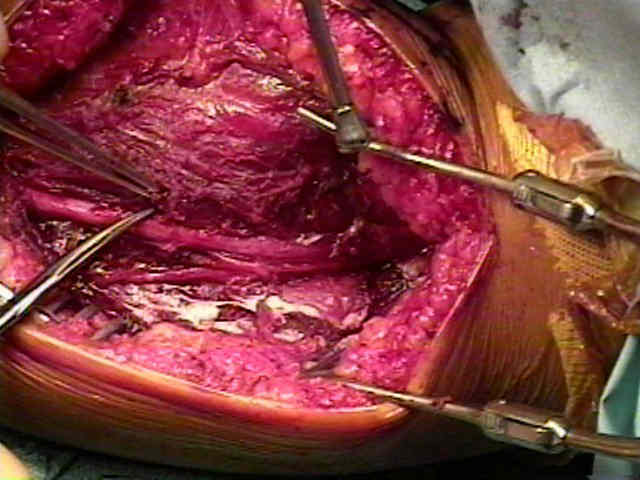
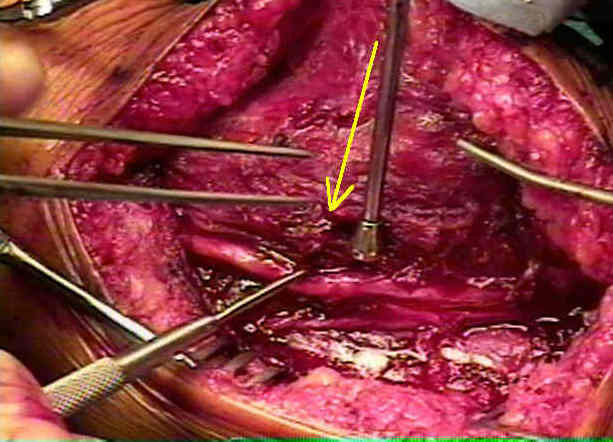
- intraoperatively, it was found that the nerve was tented over the fracture site because of the varus deformity.
-
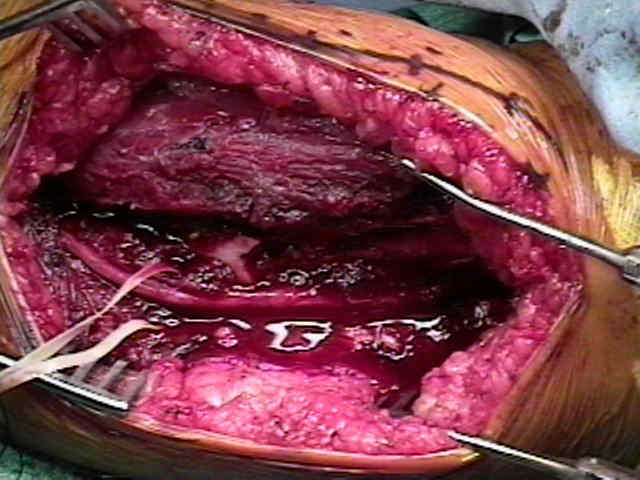
- when the deformity was corrected, traction on the nerve was relieved.





-



References
- Immediate radial nerve palsy complicating fracture of the shaft of the humerus: when is early exploration justified?
- Radial palsy in shaft fracture of the humerus.
- Treatment of fractures of the shaft of the humerus accompanied by paralysis of the radial nerve.
- Radial nerve lesions associated with fractures of the humeral shaft.
- Plate fixation of the humeral shaft for acute fractures, with and without radial nerve injuries.
- Radial nerve palsy caused by open humeral shaft fractures.
- Surgical treatment of the radial nerve lesions associated with fractures of the humerus.
- Splinting for radial nerve palsy. Colditz JC. J Hand Ther. 1987;1(1:18.
- An improved splint for radial (musculospiral) nerve paralysis.
- Radial nerve palsy associated with high-energy humeral shaft fractures.
- Radial nerve entrapment by the lateral intermuscular septum after trauma.
- Surgical treatment of the radial nerve lesions associated with fractures of the humerus.
- Treatment of humeral shaft fractures related to associated injuries. A retrospective study of 237 patients.
- Susceptibility to tourniquet-induced radial palsy in the presence of previous humeral fracture.
- Radial palsy in shaft fracture of the humerus.
- Radial nerve paralysis associated with fractures of the humerus. A review of 62 cases.
- Primary Radial Nerve Palsy in Patients With Acute Humeral Shaft Fractures.
- Radial nerve palsy associated with humeral shaft fracture. Is the energy of trauma a prognostic factor?