

- PreOp Planning: 
- tendon transfer is chiefly indicated for stage II tenosynovitis;
- subtalar joint must demonstrate nearly a full range of inversion;
- early synovectomy of the tendon sheath not only relieves discomfort but will possibly delay or prevent
attenuation or rupture;
- in presence of correctable hyperpronation, transfer of FDL tendon to distal posterior tibial tendon stump
is considered;
- if subtalar joint cannot be brought into nearly full inversion because of long-standing deformity, then tendon transfer is contra-indicated;
- in this case consider subtalar arthrodesis;
- sping ligament:
- as pointed out by Gazdag and Cracchiolo (1997), 18 out of 22 posterior tib ruptures had injury to the sping ligament;
- this ligament courses from the sustentaculum tali to the plantar surface of the navicular, and helps support the head of the talus;
- ref: Rupture of the posterior tibial tendon. Evaluation of injury of the spring ligament and clinical assessment of tendon transfer and ligament repair.
- Surgical Technique:
- position bump under contralateral hip;
- begin incision 10 cm proximal to meidal malleolus, continue distally to about 1 cm posterior to medial border of tibia, & end incision
just distal to the medial aspect of navicular tuberosity;
- deep fascia is incised, with care to preserve a portion of flexor retinaculum, and the TP is exposed, lying close to posterior margin
of the tibia;
- exposure, inspection, and debridement of tibialis posterior:
- "white sign"
- posterior tib will be visible beneath the flexor retinaculum;
- abnormally whitened appearance indicates more distal tear;
- the tendon sheath should be opened in its entirity;
- if tendon is of normal length, the tendon debridement, tenosynovectomy and sheath resection are performed;
- if tendon is elongated or appears pathologic, then FDL transfer is required;
- most tendons will not have complete rupture, but rather, will have thickening and scarring and often a longitudinal tear
will be present;
- complete ruptures tend to occur just distal to medial malleolus; 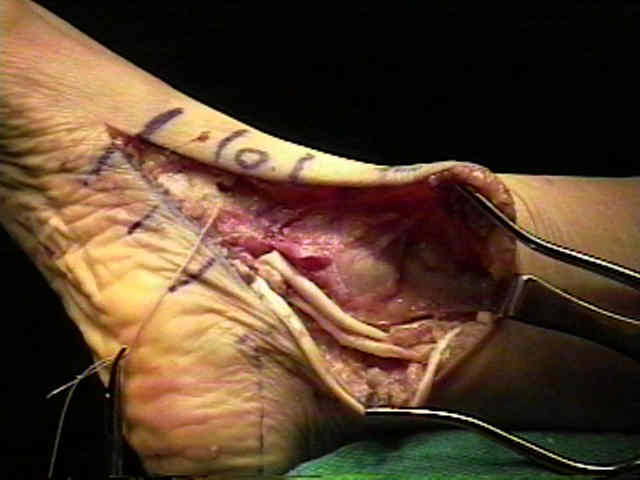
- PT tendon is transected leaving a 3 cm stump of tendon attach to the navicular;
- this tendon stump may be necessary to repair the spring ligament;
- case example: this patient had a degenerative longitudinal rent in the posterior tibialias tendon;
- spring ligament inspection:
- at this point in the case, the sping ligament is inspected;
- the superomedial portion of the spring ligament extends from the sustentaculum tali to the navicular;
- look for ligament laxity, longitudinal tears, or complete rupture;
- if the ligament cannot be repaired then use the stump of the PT tendon to augment the reconstruction;
- also consider spliting distal posterior tibial segment and achoring half to medial malleolus & other to sustentaculum;
- references:
- Spring Ligament Reconstruction Using the Autogenous Flexor Hallucis Longus Tendon
- Anatomic study of medial side of ankle base on joint capsule: alternative description of the deltoid and spring ligament.
- Spring Ligament Instability.
- Rupture of the posterior tibial tendon. Evaluation of injury of the spring ligament and clinical assessment of tendon transfer and ligament repair.
- Adult acquired flatfoot deformity at the talonavicular joint: reconstruction of the spring ligament in an in vitro model.
- Combined Spring and Deltoid Ligament Repair in Adult-Acquired Flatfoot
- What to Do with the Spring Ligament.
- Anatomical reconstruction of the spring ligament complex: "internal brace" augmentation.
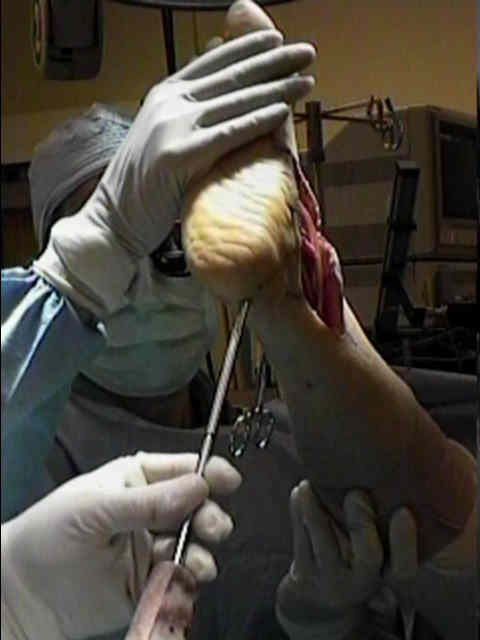
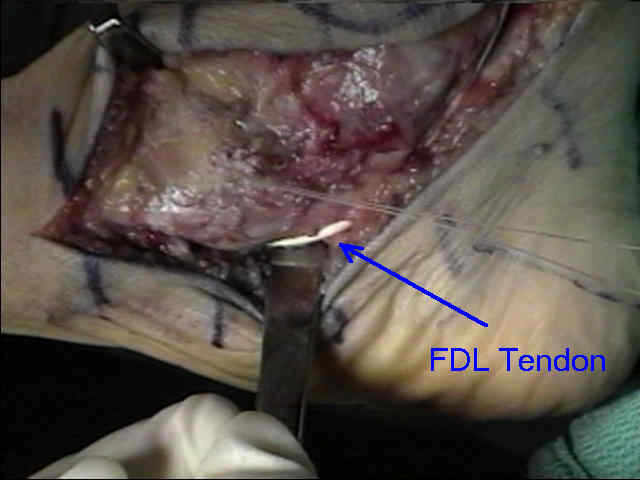
- FDL tendon harvest
- the FDL sheath is opened distally and is cut distally and is opposed to undersurface of the navicular;
- the FDL tendon sheath is found directly behind the PT tendon sheath;
- it is transected as distally as possible (usually as it crosses the FHL tendon);
- usually the biggest pitfall of the case is not obtaining enough FDL length;
- it is not necessary to tenodese the distal FDL tendon stump to the FHL since there are distal interconnections;
- ref: Risk of Neurovascular Injuries in Flexor Hallucis Longus Tendon Transfers: An Anatomic Cadaver Study
- if the PT's sheath is scarred then it is important to leave intact the FDL tendon sheath behind the medial malleolus;
- alternatively, if the posterior tib sheath is clean, the FDL tendon can be retracted and passed into the PT sheath;
- drill hole is passed thru navicular tuberosity from dorsal to plantar direction;
- FDL is brought thru the drill hole from inferior to superior;
- medial calcaneal sliding osteotomy:
- ref: The role of osteotomies in the treatment of posterior tibial tendon disorders.
Manoli A II, Beals TC, Pomeroy GC. Foot and Ankle Clin.1997;2:309-317.




- optimizing tension of the graft:
- place anke into slight varus & eqinus, and forefoot adduction;
- the ankle should not be over tightened;
- if the navicular is laterally subluxed on the talus, consider shortening the medial capsule prior to tendon suturing;
- then put tension on FDL tendon and anchor down the suture;
- if possible, suture the FDL tendon back onto itself, otherwise anchor the FDL to the stump of the PT tendon;




- misc: consider achilles tendon lengthening if necessary;
- wound closure:
- if the tibialis posterior muscle belly appears healthy w/ normal 1 cm excursion, then the tendon can be sutured to the FDL
at the level of the meidal malleolus;
- close the tibialis posterior tendon sheath with care to avoid the N/V bundle;
- Outcomes:
- in the report by Sammarco et al, 19 consecutive patients underwent FHL (FHL) tendon transfer and medial displacement
calcaneal osteotomy for the treatment of Stage 2 posterior tibial tendon dysfunction;
- FHL tendon was utilized for transfer because it approximates the strength of the posterior tibialis muscle and is stronger than
the peroneus brevis muscle;
- AOFAS hindfoot score improved from 62.4/100 to 83.6/100;
- wtbearing preoperative and postoperative radiographs revealed no statistically significant improvement for the medial
longitudinal arch in measurements of lateral talo-first metatarsal angle, calcaneal pitch, vertical distance from the floor to
medial cuneiform, or talonavicular coverage angle;
- three feet had a normal medial longitudinal arch and six feet had a longitudinal arch similar to the opposite side following the procedure;
- patient satisfaction was high: 10 patients satisfied without reservations, 6 patients satisfied with minor reservations, and 1 dissatisfied;
- no patient complained of donor deficit from the harvested FHL tendon.
- in the report by Moseir-LaClair, et al, the authors reviewed 26 patients with 28 pes planovalgus feet secondary to Johnson stage 2
posterior tibial tendon insufficiency;
- all were treated with flexor digitorum longus tendon transfer, lateral column lengthening, medial displacementn calcaneal osteotomy,
and heel cord lengthening; mean patient age at surgery was 48.5 years;
- mean follow-up to date is 5 years;
- medial cuneiform to fifth metatarsal distance improved from -0.2 mm preoperatively to 7.6 mm postoperatively;
- similarly, the talonavicular distance improved from 19.4 mm preoperatively to 10.9 postoperatively;
- there were no nonunions;
- four feet (14%) displayed radiographic signs of calcaneocuboid arthritis at follow-up;
- only one was symptomatic requiring calcaneocuboid joint fusion;
- the double osteotomy technique provides symptomatic relief and lasting correction of the pes planovalgus deformity associated
with stage 2 posterior tibial tendon insufficiency at intermediate follow-up;
- in the report by Guyton et al, the authors reviewed the results of 26 patients who had undergone the procedure at an average of 32
months prior to follow-up (range 12 to 70 months) with particular attention to objective functional parameters;
- between 1993 and 1998, 26 patients underwent FDL transfer and medial displacement calcaneal osteotomy
- all patients except three could perform a single-leg toe rise at follow-up, a maneuver none could perform preoperatively;
- of these three, two cases were technical failures with loss of fixation of the FDL transfer early in the postoperative course,
ultimately requiring revision procedures including one subtalar fusion;
- clinically assessed subtalar motion remained 81 +/- 15% of the contralateral side in those patients with unilateral disease;
- pain relief was rated excellent by 75% and good by 16%;
- function was felt to be markedly improved by all patients except the three who were unable to perform a single-leg toe rise;
- median length of time to self-rated maximal medical improvement was 10 months;
- references:
- Treatment of stage II posterior tibial tendon dysfunction with flexor hallucis longus transfer and medial displacement calcaneal osteotomy.
- Intermediate follow-up on double osteotomy and tendon transfer procedure for stage II posterior tibial tendon insufficiency.
- Flexor digitorum longus transfer and medial displacement calcaneal osteotomy for posterior tibial tendon dysfunction: a middle-term clinical follow-up.
- Long-term follow-up of flexor digitorum longus transfer and calcaneal osteotomy for stage II posterior tibial tendon dysfunction.
- Outcome of medial displacement calcaneal osteotomy for correction of adult-acquired flatfoot.
- Functional results of posterior tibial tendon reconstruction, calcaneal osteotomy, and gastrocnemius recession.
Medial arch strain after medial displacement calcaneal osteotomy: an in vitro study.
Treatment of ruptured posterior tibial tendon with direct repair and FDL tenodesis.
Shereff MJ. Foot Ankle Clin. 1997;2:281-296.