

- Anatomy:
 - MCL is composed of superficial & deep portions;
- MCL is composed of superficial & deep portions;
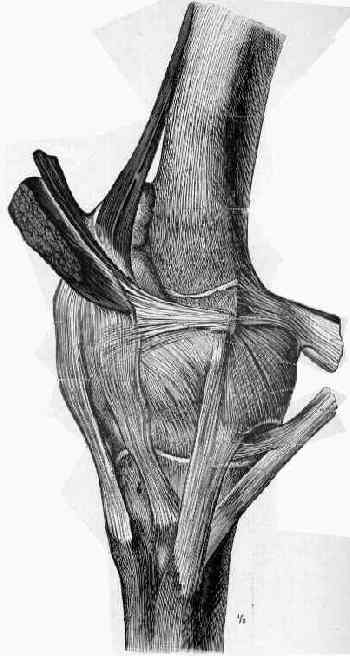
- superficial MCL:
- anatomically this is the second (middle) layer of the medial compartment;
- proximal attachment: posterior aspect of medial femoral condyle;
- 3.2 mm proximal and 4.8 mm posterior to the medial epicondyle
- distal attachment:
- metaphyseal region of the tibia, upto 4-5 cm distal to the joint, lying beneath the pes anserinus;
- two tibial attachments
- anterior arm of the semimembranosus tendon and about of 12.2 mm distal to the tibial joint line
- broad insertion of about 61.2 mm distal to the tibial joint line; it is located just anterior to the posteromedial crest of the tibia;
- ref: The Anatomy of the Medial Part of the Knee
- function: provides primary restraint to valgus stress at knee;
- providing from > 60-70% of restraining force depending on knee flexion angle;
- at 25° of flexion, the MCL provides 78% of the support to valgus stress;
- at 5° of flexion, it contributes 57% of the support against valgus stress;
- superficial ligament can be divided into anterior & posterior portions;
- anterior fibers of superficial portion of ligament appear to tighten w/ knee flexion of 70 to 105 deg;
- posterior fibers form the posterior oblique ligament:
- deep MCL:
- anatomically this is the third (deep) layer of the medial compartment, which is many cases will be separated from the superficial MCL
(layer II) by a bursa (which allows sliding of the tissues during flexion);
- divided into meniscofemoral and meniscotibial ligaments;
- inserts directly into edge of tibial plateau & meniscus;
- firmly attaches to the meniscus but does not provide significant resistance to valgus force;
- Exam Findings:
- see: valgus stress test:
- clinical findings may be subtle even with complete injury;
- it is helpful to anchor the thigh on the table w/ the knee and leg off the the edge of the table;
- opening of 5-8 mm compared to opposite knee may indicate complete tear;
- determine the point of maximal tenderness to determine whether the tear has occurred proximally, mid-substance, or distally;
- instability in slight flexion:
- anterior portion of the medial capsular is primary stabilizer at 30 deg of flexion;
- hence at 30 flexion, testing is specific for just MCL;
- instability in extension:
- posterior portion of the MCL, posterior oblique ligament, ACL, medial portion of posterior capsule & possibly PCL;
- ref: Collateral Ligament Laxity in Knees: What Is Normal?
- location of tears:
- femoral tear:
- if ligament is avulsed from medial epicondyle, ligament may elevate a small bony fragment with it, in which case, point of origin becomes tender to palpation;
- mid substance tear:
- if ligament is torn at its midpoint, tendon and overlying soft tissue may be shredded;
- in that event, defect becomes palpable and there is tenderness at the level of the medial joint line;
- tibial tear:
- tenderness may be felt 6-8 cm down medial tibial shaft (along length of the ligament insertion);
- when distal end of MCL is torn in area of pes anserinus, one may restore normal tension to this portion of MCL by securing the lower end to
freshened area of bone w/ sutures or a staple advanced distally;
- X-ray:
- Pellegrini-Stieda Phenomenon: w/ chronic injury, it is common to see calcification at origin of MCL;
- ref: Pellegrini–Stieda Syndrome.
- MRI:
- helpful for delineating of disruption of the collateral complex;
- need to determine whether injury is proximal, mid substance, or distal;
- need to determine whether the deep and/or superficial ligament is disrupted;
- collateral ligament is best visualized on T2 weight images:
- as a high signal of edema and hemorrhage in the substance of the low signal ligament;
- look for concomitant meniscal tear;
- Non Operative Treatment:
- optimum healing of the medial collateral ligament occurs when the torn ends are in contact;
- healing potential is directly related to size of the gap between the torn ends;
- healing of extra-articular ligaments is analogous to healing of other soft tissue structures, thru production and remodeling of scar tissue;
- maturation of scar occurs from 6 weeks to upto one year;
- although the maturing scar tissue has only about 60% of the strengh of the normal MCL, ultimate load to failure is unchanged (since the amount of
scar tissue is larger than original ligamentous tissue);
- references:
- Nonoperative management of complete tears of the medial collateral ligament of the knee in intercollegiate football players.
- Long-term results of conservatively treated medial collateral ligament injuries of the knee joint.
- combined ACL/ MCL injuries: (see anteromedial instability)
- w/ concomitant MCL and ACL tears, most surgeons now recommend ACL reconstruction after the valgus stability has returned;
- the one exception might be the MCL tear arising from the tibial insertion;
- references:
- Reconstruction of the anterior cruciate ligament alone in the treatment of a combined instability with complete rupture of the medial collateral ligament. A prospective study.
- Combined injuries of the anterior cruciate ligament and medial collateral ligament of the knee. Effect of treatment on stability and function of the joint.
- Operative Treatment:
- surgical plan depends on whether injury is proximal, mid substance, or distal;
- femoral avulsion:
- w/ femoral avulsion, it is important to remember that reattachment anterior to its orgin may limit knee flexion, where as posterior
placement may cause ligament laxity;
- the knee should be held flexed at 30 deg and held in varus when the ligament is reattached;
- references:
- Operative versus non-operative treatment of recent injuries to the ligaments of the knee. A prospective randomized study.
Ligamentous and capsular restraints preventing straight medial and lateral laxity in intact human cadaver knees.
Medical restraints to anterior-posterior motion of the knee.
The supporting structures and layers on the medial side of the knee: an anatomical analysis.
Classification of knee ligament instabilities. Part I. The medial compartment and cruciate ligaments.
Injuries to the Medial Collateral Ligament and Associated Medial Structures of the Knee