

 - Discussion:
- Discussion: - anterior longitudinal incision allows full exposure of the proximal tibia;
- this incision allows exposure of both medial & lateral aspects of joint w/o the necessity
for large skin flaps;
- this incsion has advantage that it leaves strong cuff of fibrous tissue attached to vastus
medialis obliquus muscle;
- this strong cuff facilitates suture placement and secure closure at the end of the case;
- straight incisions are less disruptive to the blood supply to knee than curved incisions;
- a gentle medially curved incision is an alternative which may heal with less prominent scarring and may better facilitate
knee flexion (because of less scar contraction);
- hazards:
- small medial or hockey stick incisions usually do not present a problem;
- w/ longitudinal parallel scars, it is important to avoid lateral skin flaps, and therefore lateral scars should be re-used;
- infra-patellar branch of saphenous nerve:
- Neuroma of infrapatellar branch of the saphenous nerve a cause of reversible knee stiffness after total knee arthroplasty
- Technique:
- tourniquet considerations:
- leg is optimally exsanguinated inorder to reduce residual venous stasis and to reduce chances of venous thrombosis;
- goal is to use the lowest tourniquet pressure possible;
- references:
- Vascular injuries in TKA. A review of the problem with special reference to the possible effects of the tourniquet.
- TKA after ipsilateral peripheral arterial bypass graft: acute arterial occlusion is a risk with or without tourniquet use.
- Total knee arthroplasty in patients with peripheral vascular disease
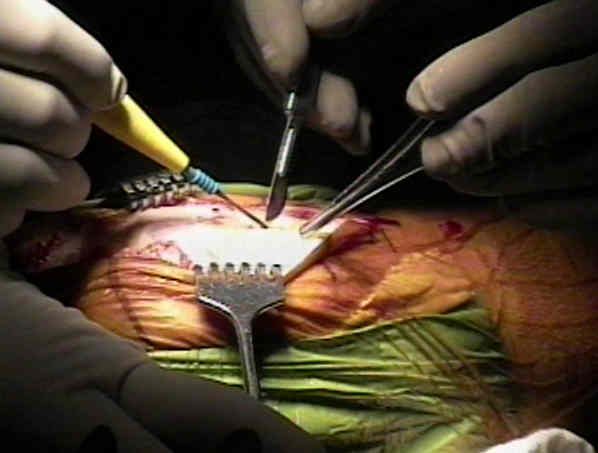
- incision considerations:
- expose the knee joint thru a straight longitudinal incision beginning 6-12 cm proximal to superior pole of the patella,
extending over patella, & ending at the medial border of tibial tuberosity or approx 6 cmm distal to the inferior pole
of the patella;
- some surgeons prefer to vary the incision w/ a gentle medial curve over patella, arguing that curved incision is less likely
to scar and contract;
- consider carrying incision upto 12 cm from superior pole of patella & carry it inferiorly an equal distance below
inf margin of patella;
- this reduces degree of skin retraction and lowers risk of tissue necrosis;
- references:
- Hypesthesia after Anterolateral versus Midline Skin Incision in TKA: A Randomized Study
- Incision stretching in primary TKA: what is the real length of our approach?
- DO PREVIOUS SCARS AROUND THE KNEE MATTER IN TOTAL KNEE ARTHROPLASTY?
- superficial retinaculum:
- after incising skin & subQ fat, it is important to sharply dissect down onto superficial retinaculum w/o undermining
above this layer;
- this preserves the subfascial vessels, decreasing risk of skin slough;
- generally, the surgeons knife will incise thru a portion of the superficial retinaculum while incising thru the subQ layer;
- at this point, insert curved Mayo's thru this defect and spread underneath both proximally and distally;
- further mobilize this layer and the gently separate the retinaculum from the underlying deep fascia using the dull end of the
scapel;
- undermining is performed medially until the fascia is elevated 5 mm past the patella;
- excessive lateral undermining may cause necrosis of skin overlying patella (esp if lateral retinacular release is
performed later in case);
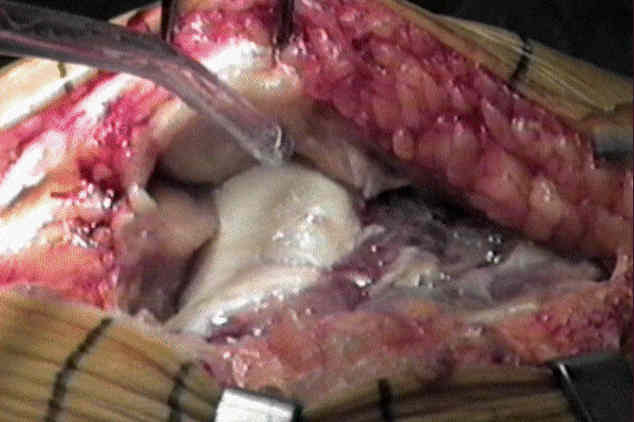
- Quadriceps and Patellar Tendon Incision:
- at proximal apex of incision, incise thru medial 1/3 of quadriceps and continue deep incision distally to superior border of patella;
- continue the incision tightly along the medial border of the patella down to the superior border of the patellar tendon;
- preserve a narrow margin of capsule on patella to make wound closure easier
- continue the incision distally thru the medial third of the patella tendon down to the tibial tubercle;
- this technique offers tremendous exposure of the knee, and allows easy eversion of the patella;
- it is essential not to disturb the insertion of the medial patellar tendon insertion;
- lower part of incision should not extend below tibial tubercle inorder, to avoid damaging infrapatellar branch of
saphenous nerve;
- transect the fat pad in line with the primarily capsular incision;
- mid-vastus arthrotomy:
- advantage over the standard incision is that the vastus medialis insertion into the medial border of the quadriceps tendon
(allows rapid restoration of extensor mechanism);
- vastus medialis muscle is divided in its mid-substance in the direction of its fibers;
- incision is made with the knee in flexion (automatically retracts transected tissues and places tension on tissues about
to be cut);
- incise thru the superficial retinaculum but leave a thin layer of fascia over the VMO;
- w/ the knee in full flexion, split thru the tendon at the superomedial corner of the patella, but do not split more than 4 cm;
- release the capsular folds of the suprapatellar pouch proximal to the patella, and evert the patella;
- references:
- V-Y quadricepsplasty in total knee arthroplasty.
- Subvastus (Southern) approach for primary total knee arthroplasty.
- Evolution of the quadriceps snip.
- Surgical technique of the midvastus arthrotomy.
- Comparison of vastus-splitting and median parapatellar approaches for primary TKA: a prospective, randomized study.
- A Comparison of Subvastus and Midvastus Approaches in Minimally Invasive Total Knee Arthroplasty
- Does the length of incision in the quadriceps affect the recovery of strength after total knee replacement? a prospective
- Excision of Fat Pad:
- use the back end of the scapel to bluntly separate the potential space between the fat pad and the patellar tendon;
- once this space has been defined, use to knife to completely remove the fat pad;
- reference:
- Scintigraphic determination of patellar viability after excision of infrapatellar fat pad and/or lateral retinacular release in TKA.
- Inverted V Capsular Incision:
- may be indicated in revision cases or when there is difficulting in everting the patella;
- inverted V capsular incision w/ 2nd arm of inverted V begins at proximal apex & extends at 45 deg angle across quadriceps
tendon, through vastus lateralis tendon, & into portion of iliotibial band;
- incision should stop short of sup. lateral geniculate artery;
- release decreases tension on patellar ligament & allows eversion of patella in almost all patients, regardless of previous
surgery;
- it is crucial not to avulse the patellar ligament from tubercle
Wound problems in total knee arthroplasty.
Intramuscular Hematoma Following a Midvastus Approach During Primary Total Knee Arthroplasty