- See: Axillary Approach to the Shoulder
- Indications:
- most often used for Bankhart repairs for anterior shoulder dislocations;
- Positioning: beach chair w/ full access to posterior aspect of shoulder;
- Incision:
- incision is placed in major axillary skin fold;
- skin incision begins in the axilla and is centered over pectoralis major tendon (usually no longer than 6 cm);
- if incision needs to be extended, extend it toward coracoid;
- cephalic vein marks the location of the deltopectoral interval;
- split in deltopectoral interval continues along medial aspect of cephalic vein down the clavipectoral fascia; - the cephalic vein proceeds superiorly over the coracoid.


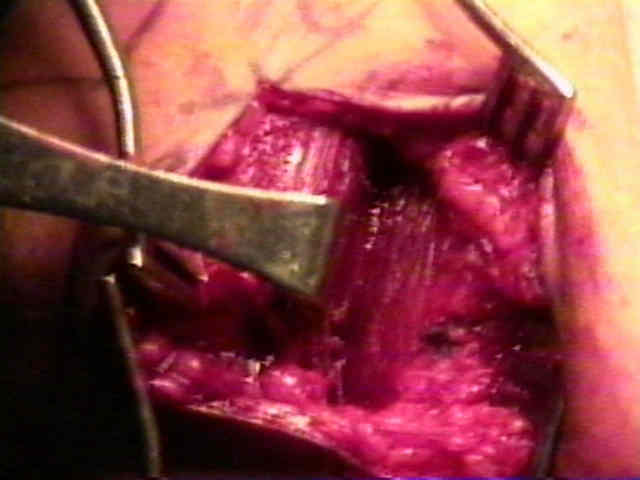
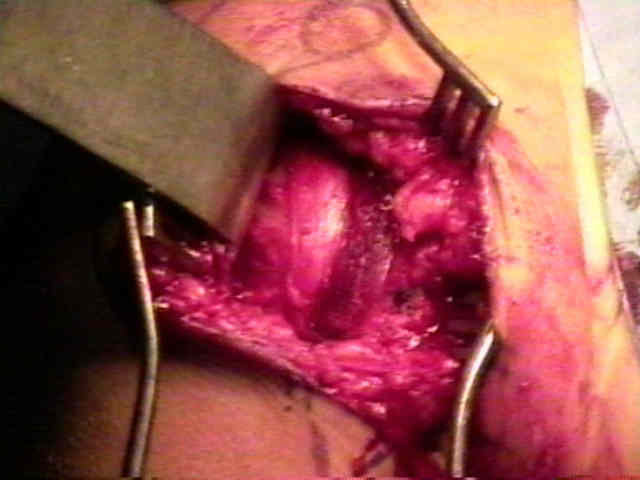
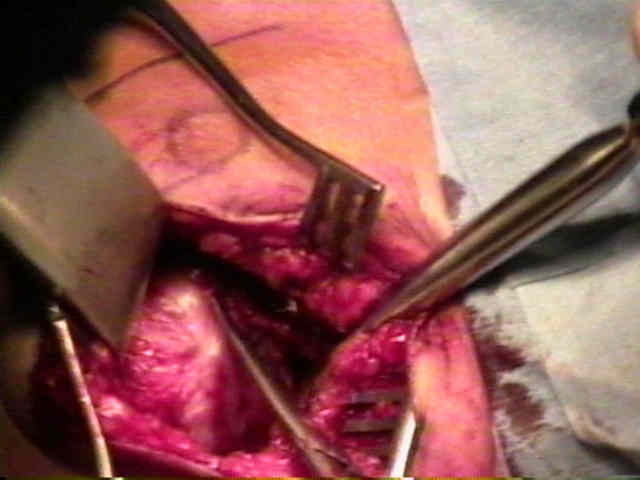
- Deep Exposure: - elevate deep surface of deltoid;
- laterally this will enter into subacromial bursa;
- tip of the coracoid and the conjoined tendon (short head of biceps and the coraco-brachialis) is identified;
- clavipectoral fascia is differentiated easily from the deeper tissues, because it will not move with internal and external rotation;
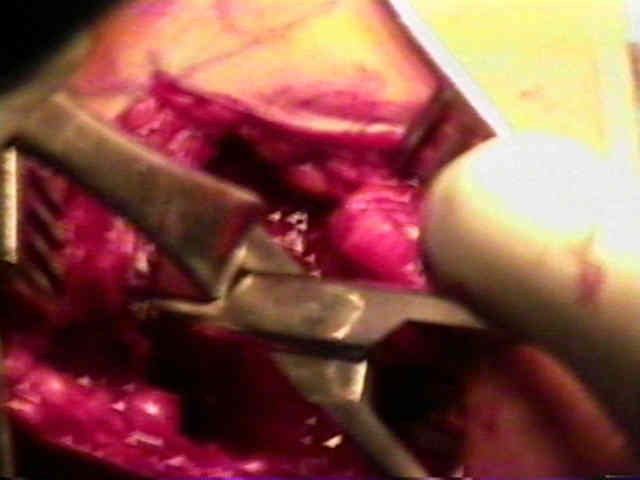

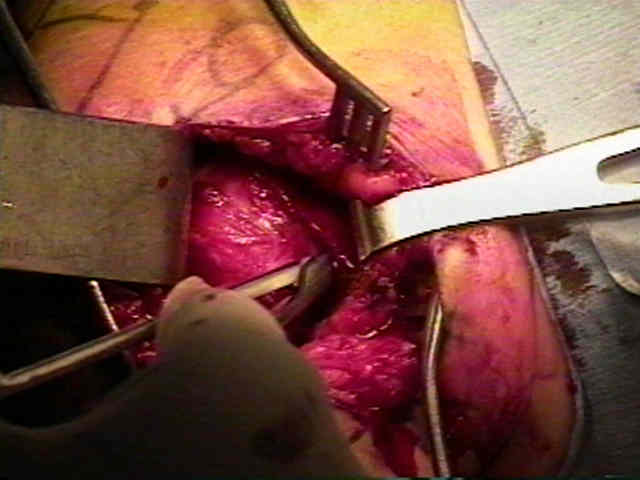
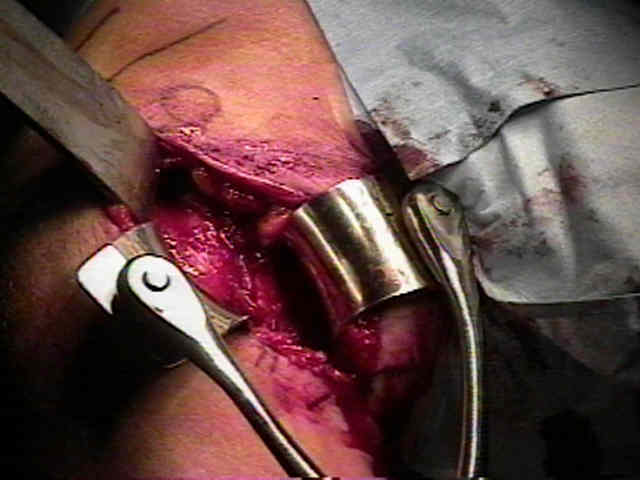
- next the Charnley type retractors are inserted;
- blades are placed deep to the deltoid and the conjoined tendon;
- inner limb of the Balfour should be just caudal to the coracoid tip;


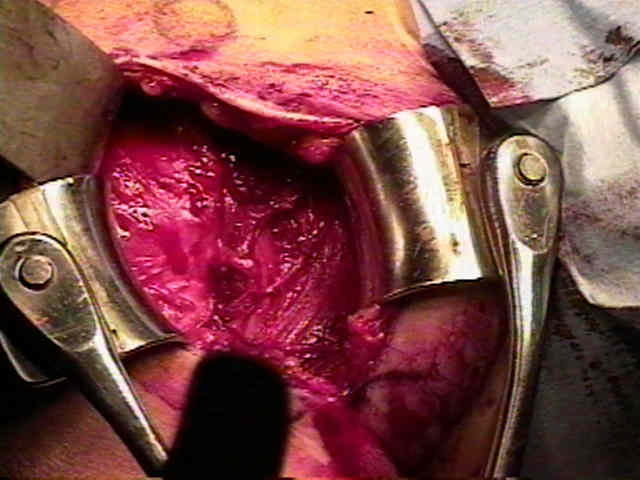
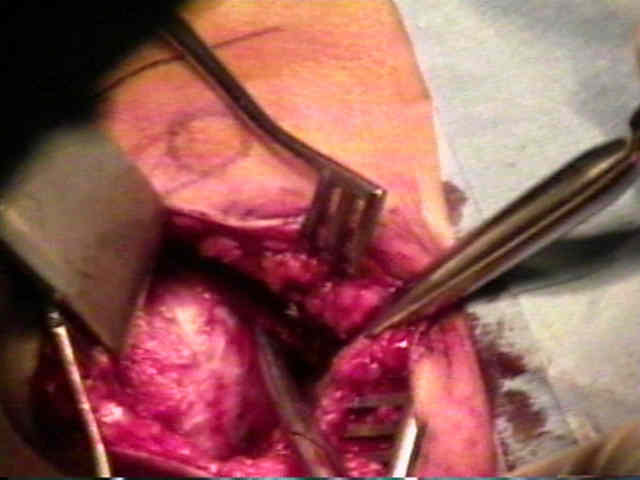
- Preparation for Subscapularis Transection:
- identify the anterior humeral circumflex vessels (three sisters);
- identify the axillary nerve at the inferior aspect of subscapularis as it courses toward quadrangular space;
- here the nerve is joined by posterior humeral circumflex vessels;
- before an incision is made in the subscapularis, the arm should be externally rotated to avoid damage to axillary nerve and circumflex vessels;
- finally, prior to incision, insert two or three tagging sutures just medial to the proposed line of transection, which will facilitate retraction;
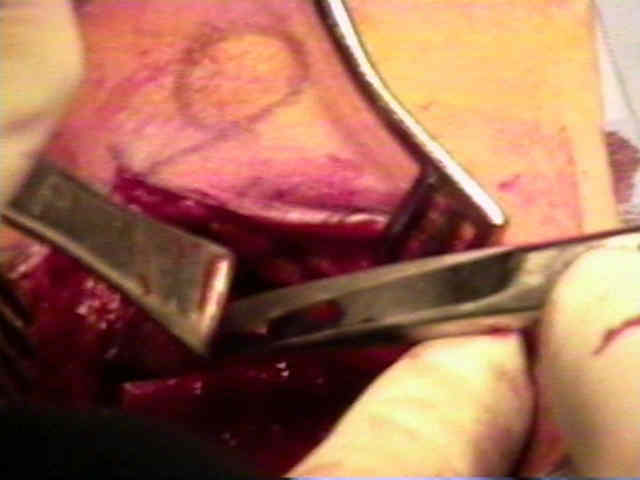
- Subscapularis Transection:
- enter glenohumeral joint over superior border of subscapularis and slightly lateral to biciptal groove;
- a vertical incision is made thru the subscapularis tendon and capsule which follows a Joker elevator, which has been inserted from above and which is aligned with the articular margin;
- 1 cm of capsule and tendon is left attached to the lesser tuberosity to facilitate subscapularis closure;
- inferior margi of the muscle is left intact, as is AHCA, which will help protext the axillary nerve


- Articular Exposure:
 -
-
-----------------------------