

- See: Bone Tumor Menu:
- Osseous Sarcoma:
- occur less often in bone than in soft tissue;
- occurs in older patient population & may arise out of Pagets Dz or from a bone infarct (such as sickle cell);
- it usually presents as an aggressive stage IIb sarcoma;
- pathologic frx may be the presenting feature;
- has a high rate of metastasis, especially to regional lymph nodes.
- Soft Tissue Sarcoma:
- most common soft-tissue sarcoma in adults;
- it is heterogeneous tumor w/ respect to histology & prognosis;
- malignant cells are of histiocytic derivation;
- early osseous invasion & metastases to regional lymph nodes is common;
- Clinical Presentation:
- presents in adults;
- may present as large mass involving deep soft tissues of proximal limbs;
- may present as a small, superficial, low grade tumor in the distal limbs;


- Radiographs:
- bony lesions will show destructive changes w/ cortical erosion and a poorly defined, permeative margin.
- when associated with a radiodense bone infarct, MFH may be misinterpreted as sarcomatous transformation of enchondroma;
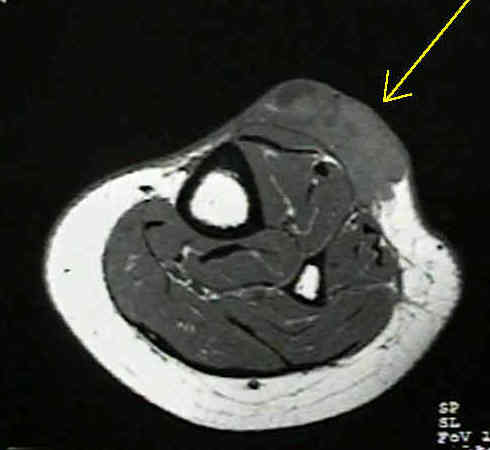
- CT/MRI:
- mixed density signal
- areas of internal hemorrhage
- areas of myxoid density (signal)
- occasionally lobular growth;
- Bone Scans:
- show increased uptake in adjacent cortex;
- Histologic Characteristics:
- include mixture of fibrous tissue arranged in storiform pattern;
- areas filled with large, foamy histiocytes;
- scattering of wildly bizarre, atypical cells w/ obvious mitotic figures.
- cellular necrosis & vascular invasion;
- Paraneoplastic syndromes:
- eosinophilia
- hypoglycemia
- fever
- abnormal LFTs
- Pathology: a pleomorphic, high grade, bimodal sacroma in which the only differentiating feature is collagen;
- Gross:
- lobular growth pattern
- reactive capsule
- varying amounts of fat
- Histologic types:
- Atypical fibroxanthoma
- occurs only in the skin
- mixture of pleomorphic and storiform areas
- identical to the deep pleomorphic lesion
- nodules or ulcers 2 cm or less
- almost invariably a benign course;
- Storiform-Pleomorphic
- majority of cases (70%)
- occur deep
- mixture of plumb spindle cells and histocytes
- cartwheel or fascicular collagen
- modest numbers of xanthoma cells
- modest numbers of inflammatory cells
- high mitotic activity
- multinucleated giant cells;
- focal areas of myxoid change
- focal areas of osteoid;
- Myxoid MFH (25%)
- like above but greater than 50% myxoid areas
- differential diagnosis benign myxoma or myxoid variant of other sarcomas
- Staging:
- Chest CT
- Abdominal/Pelvic CT (12% incidence of nodal metastasis)
- bone or gallium scan
- CT or MRI of lesion;
- Treatment:
- attention is directed to ruling out metastases to the regional lymph nodes;
- low grade stage I tumors usually develop in more peripheral & superfical locations than do high grade tumors.
- treatment w/ wide surgical excision is usually adequate, w/ amputation reserved for multiple recurrances.
- stage II tumors require excision w/ wide margins or amputation;
- preop XRT or postoperative chemo, or both, may be indicated;
- Chemotherapy:
- chemotherapy in association with surgery may improve survival for patients with malignant fibrous histiocytoma of bone;
- Results: 5 yr mortality
- pleomorphic - 55% (most common type)
- giant cell - 55%
- myxoid - 23%
- inflammatory - 33%
Surgical treatment and prognosis in patients with high-grade soft tissue malignant fibrous histiocytoma of the extremities
Adjuvant chemotherapy for malignant fibrous histiocytoma in the femur and tibia.
Malignant fibrous histiocytoma of bone
Hereditary bone dysplasia with malignant change. Report of three families.
Malignant fibrous histiocytoma of the soft tissues of the trunk and extremities.