


- Landmarks: 
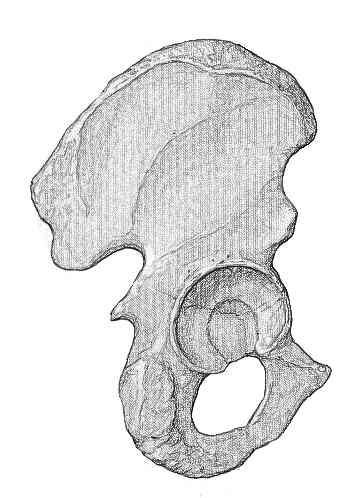
- posterior superior iliac spine: forms the superior landmark;
- incision starts at the posterior 1/3 of the greater trochanter and extends proximally for 10 cm toward a point 2 fingerbreadths below the PSIS;
- this will bring the incision directly over the sciatic notch and will also place it parallel to fibers of gluteus maximus;
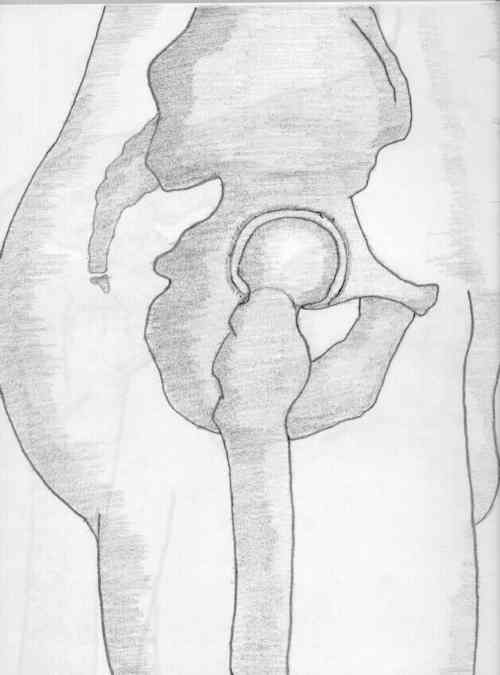
- greater trochanter: forms central landmark for incision & its posterior edge is prominent and usually easily palpable;
- while posterior aspect is free of muscles, its anterior & lateral aspects are covered by tensor fascia lata & gluteus medius muscles;
- incision is centered over the posterior 1/3 of the proximal trochanteric tip, but more distally
the incision must be centered over the midportion of the femoral shaft;
- distal landmark: formed the mid aspect of the femoral shaft;
- incision is extended from the posterior third of the trochanter to a point 10 cm distal, centered over the shaft of the femur;
- the incision needs to be made distal enough, in order to allow exposure of the lesser trochanter;
- Technique:
- place the leg in 60 deg of flexion, and draw out the landmarks as outlined above;
- once the landmarks are marked out, don't reposition the leg because the greater trochanter and the femoral shaft will change position relative to the overlying skin;
- if the landmarks are placed with the leg in flexion, but the incision is made with the leg in extension, then the dissection
will procede posterior to the greater troch and shaft;
- marking out the incision w/ the hip flexed to 90 deg will often place the proximal portion of the incision too far posteriorly;
- w/ the hip flexed to 60 deg and make a straight longitudinal incision connecting the PSIS, posterior third of the greater trochanter
and the mid aspect of the femoral shaft;
- Special Considerations:
- if a trochanteric osteotomy is required, then the proximal incision should be made toward the PSIS rather (than 2 fingerbreadths below it), in order
to allow superior displacement of the greater trochanteric fragment;
- in most cases, there are no consequences of incising thru previously made hip incisions;
- most orthopaedists cannot recall a single case of wound necrosis resulting from incising thru old incisions;
- in young muscular patients, the gluteus maximus fibers may encroach more anteriorly into the IT band as compared to older patients;
- in these patients, an incision which is too posterior will likely encroach into the maximus;
- obese patients:
- a larger and more posteriorly biased incision is required;
- the more posteriorly biased incision allows easier access for broaching of the femoral canal;
- Pitfalls:
- incision too far posterior:
- this often results from incisions that are placed slightly posteriorly, but are then brought further posteriorly during the dissection thru the SubQ tissues;
- making a straight skin incision w/ the leg flexed 90 deg will often place the proximal portion of the incision too far posteriorly;
- as the dissection proceeds thru the SubQ tissue, palpate for the greater trochanter and direct the deep incision anteriorly if needed;
- above the level of the trochanter the iliotibial band thins out rapidly in a posteroir direction;
- hence incisions placed to far posteriorly, will result in extensive splitting of the gluteus maximus,
which causes increased bleeding and possible denervation of the anterior maximus;
- even if the incision has been made too far posterior, there is usually little difficulty in exposing the femur and the acetabulum;
- incision too far anterior:
- this is an uncommon mistake, but when it occurs, there is difficult with exposure of the acetabulum
The trochanteric approach to the hip for prosthetic replacement