- Discussion:
- precise AP & Lateral projections are required to evaluate normal anatomic relationships;
- there should be no rotation to the forearm;
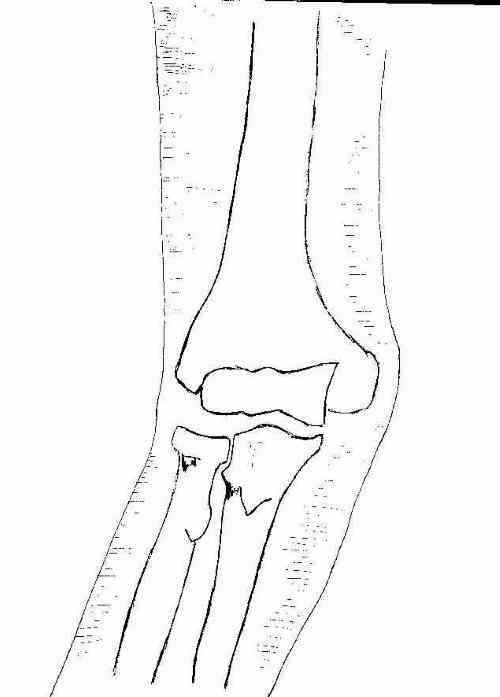
- AP View:
- medial and lateral epicondyles and humeral-ulnar/radial articulation;
- carrying angle;
- if flexion contracture is present, 2 AP views should be taken, one perpendicular to the forearm and one perpendicular to the humerus;
- technique: AP
- forearm is positioned supine (palm up) on the table;
- elbow joint is fully extended and the fingers slightly flexed;
- central beam is directed perpendicular to the elbow joint;
- AP views with the beam perpendicular to the proximal forearm and perpendicular to the distal humerus should be obtained;
- Lateral View:
- forearm flexed to 90;
- line from radial head to capitulum;
- film should demonstrate trochlea & capitellum overlapping w/ space between the humerus and the radial head; 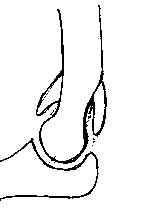
- soft tissue structures:
- anterior fat pad:
- superficial part of anterior fat pad should be in front of coronoid fossa;
- in normal elbow the anterior fat pad should be barely visualized;
- look for small radiolucent area between bony rim & moderate opaque shadows of brachialis;
- w/ joint effusion (2nd to a minimally displaced radial head frx) there will be anterior & superior displacement of anterior fat pad;
- posterior fat pad should not be seen at all;
- technique:
- forearm rests on its ulnar side on cassette w/ elbow flexed 90 deg;
- central beam is directed vertically toward the radial head;
- Internal oblique:
- trochlear notch of ulna and tip of olecranon process;
- shows medial epicondyle and coronoid process of ulna;
- External oblique:
- capitulum and head of radius; proximal radioulnar joint
Radial head-capitellum view: an expanded imaging approach to elbow injury.
Assessment of the radial head-capitellum view and the dorsal fat-pad sign in acute elbow trauma.
Critical evaluation of the radial head-capitellum view in acute elbow with an effusion.