

- Discussion:

- used in conjunction w/ a posterior approach: for fixation of condylar fractures, as well as exposure of distal humeral non unions;
- olecranon osteotomy can be either non-articularl or trans-articular;
- usually the non-articular olecranon osteotomy is used for non-articular condylar fractures;
- trans-articular osteotomy is reserved for articular condylar fractures;
- Intra-articular Osteotomy: 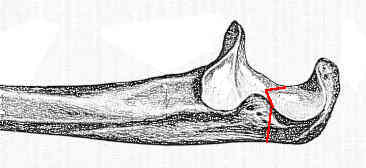
- as always first elevate the ulnar nerve;
- before performing olecranon osteotomy, its wise to predrill proximal ulna;
- 1 cm longitudinal incision is made in the midline of the triceps;
- 4.5 mm drill is used to make glide hole in proximal frx fragment;
- golf tee is inserted, and 3.2 mm drill is inserted across distal fragment;
- 6.5 mm tap is inserted across the frx site;
- the hole is tapped until resistance is felt, which also marks the proper depth of the 6.5 mm cancellous screw;
- elevate the aconeus off the olecranon to expose the articular surface;
- a sponge may be placed across the articular surface for proctection;
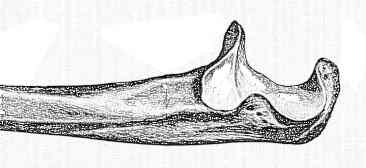
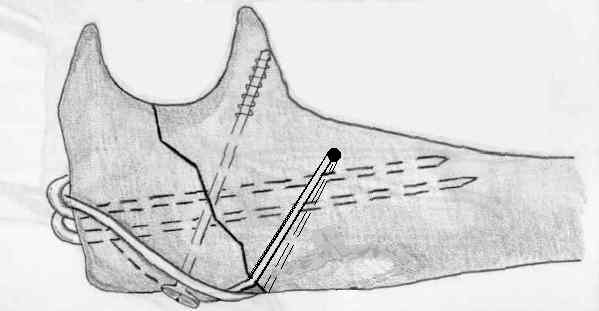
- intra-articular chevron olecranon osteotomy is then performed w/ oscillating saw perpendicular to long axis of ulna 3-4 cm proximal to its tip;
- the chevron osteotomy prevents rotational malalignment;
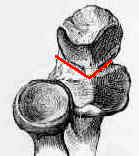
- osteotomy is made in center of olecranon sulcus because this area of olecranon has least amount of articular cartilage;
- the hyaline cartilage of the proximal ulna is not continuous, but rather lacks cartilage w/ in the mid portion;
- this is the optimal position for olecranon osteomy;
- see: anatomy of olecranon;
- chevron osteotomy is created a w/ thin oscillating saw until the far subchondral surface is reached;
- the osteotomy should be completed w/ thin-bladed osteotome which cracks articular surface of semilunar notch;
- cut is completed with osteotome using tension break of articular cartilage and subchondral bone;
- a freer elevator may be placed over the articular surface for protection;
- Elevation of Extensor Mechanism:
- residual portions of the capsule are removed;
- as triceps is elevated on both medial and lateral sides, a small margin of triceps should be left on either side to allow for suture repair at completion of case;
- proximal part of olecranon may then be elevated w/ triceps, which provides exposure as far as 7.5-10 cm above joint line before radial nerve is threatened
on the lateral side of the exposure;
- usually the branch to the brachioradialis will be encountered first;
- see: posterior approach to the elbow;
- further exposure is obtained by subluxation of the joint;
- Osteotomy Fixation:
- 6.5 mm cancellous bone screw (over washer) in combination with a figure of 8 wire may be utilized for fixation of the olecranon osteotomy;
- the proper screw length is based on the insertion depth of the 6.5 mm tap as it achieves moderate torsional resistance;
- in small ulna, screw thread may not pass into meduallary cavity of shaft and a long 6.5 mm cancellous bone screw may jam before it achieves a good bite;
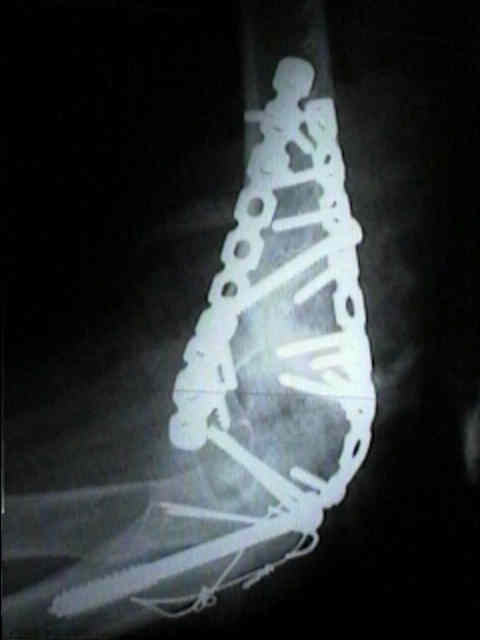
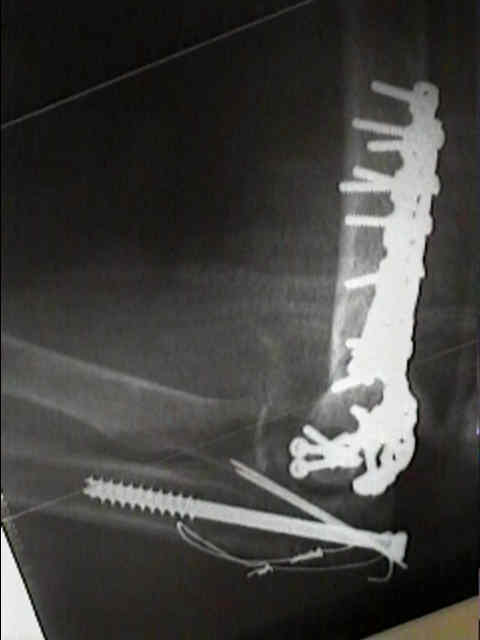
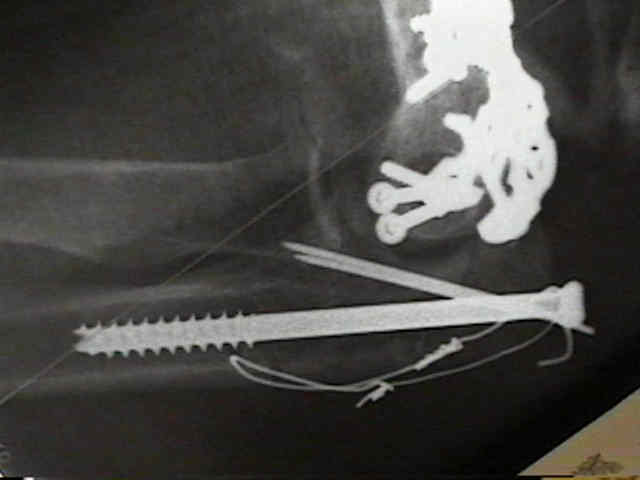
- Alternative Fixation:
- secure osteotomy w/ two oblique 0.045-in (1.143-mm) smooth K wires & tension-band wire;
- proximal ends of the K wires are carefully bent and anchored into bone;
- tension wire is placed through a drill-hole in the ulna distal osteotomy and passed under K wires and triceps proximally to create tension band;
- Disadvantages of Osteotomy:
- disadvantage is that osteotomy must be stabilized at conclusion of operative procedure;
- non-union of olecranon osteotomy may occur upto 5 % of cases;
- osteotomy hardware is often painful, requiring removal
The proximal ulna: An anatomic study with relevance to olecranon osteotomy and fracture fixation.
Olecranon Osteotomy for Exposure of Fractures and Nonunions of the Distal Humerus.