

- Discussion:
- see: lag screw theory:
- when the fibular fracture is sufficiently oblique, is not comminuted, and is not osteoporotic, then sufficient fixation can be achieved w/ only two lag screws;
- the oblique fracture should be longer than 2x diameter of bone inorder for the fracture to be fixed with 2 lag screws alone;
- when these criteria are not met, then application of a lateral plate will be necessary;
- advantages:
- allows for a smaller incision;
- the hardware is not prominent and usually does not have to be removed;
- lag screws will not interfere w/ syndesmotic screws (if they are needed);
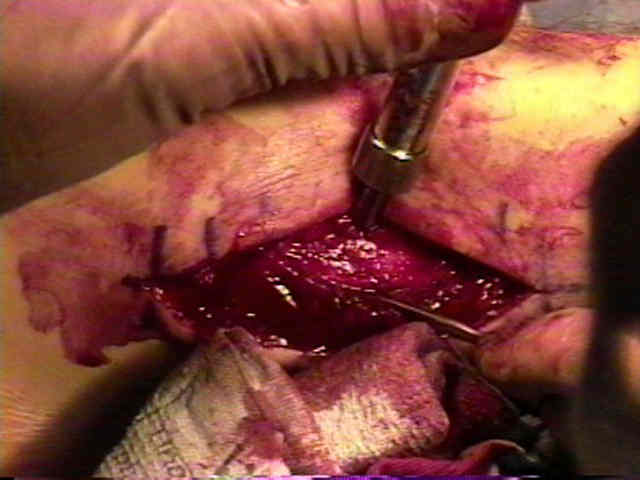
- Technique:
- flouroscopy is required if there is a concomitant syndesmotic injury
- generally lag screws are inserted from anterior to posterior to produce intrafragmentary compression;
- 3.5 mm cortical screw are used most often, but 2.7 mm screws can be used in smaller patients;
- after reduction, fracture is fixed with 1 or 2 lag screws, using standard techniques;
- it is essential that the reduction clamps be locked in a stable position, which will not interfere w/ the drill;
- also note that the anterior fibula is shaped like a narrow mountain ridge;
- ensure that enough soft tissue has been stripped at the gliding holesite, so that the drill position is perfect;
- if two lag screws are to be used, then insert both screws in a position midway between perpendicular to the bone and perpendicular to the fracture;
- this will "create more room" for both screws;
- it is important to avoid splitting the posterior spike on the distal fragment;
- if only one lag screw is to be inserted then place it perpendicular to the fracture line for maximal compression;
- when only one lag screw is used, then it will be necessary to apply a 1/3 tubular plate inorder to neutralize rotational & axial forces on the fibula;
- apply the countersink to make the screw head to improve seating on the anterior fibula and to make the head less prominent;
- the countersink will cause the screw to sink deeper, causing it to be more proud;
- screws must engage the posterior cortex for secure fixation but must not protrude far enough posteriorly to encroach on the peroneal tendon sheaths;
- often lag screws are overmeasured and appear proud on postop x-rays;
- when a proud lag screw is recognized intraoperatively, the surgeon may find that replacing the screw with a smaller one does not achieve the same screw bite;
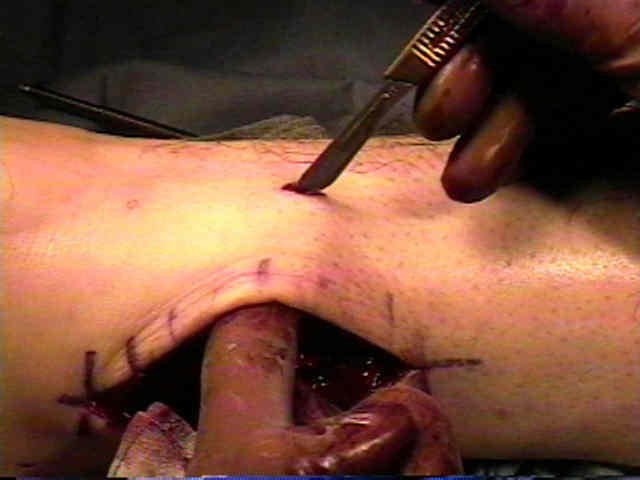
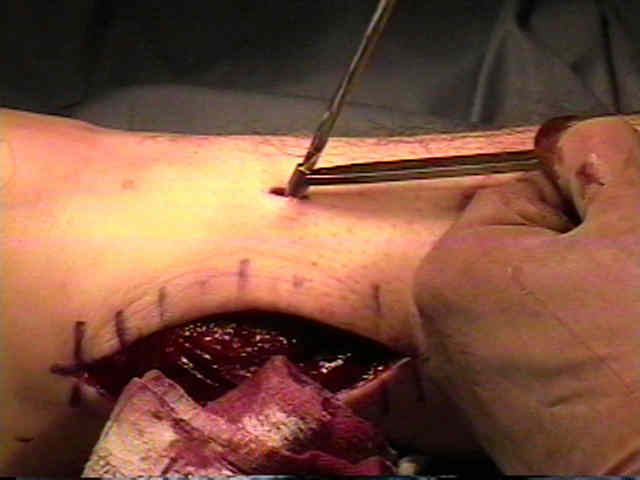
- Alternative Technique:
- if the incision is slightly posterior, it may be difficult to place the lag screw due to the tightness of the soft tissues anteriorly;
- a solution to this problem involves creation of a stab incision directly in line with the proposed site of lag screw insertion;
- Case Examples:
- preoperative AP, mortise, and lateral views:



- postoperative films demonstrating an anatomic reduction:















