


- Discussion:
- to evaluate C1 (Jefferson), Dens, superior facets of C2;
- for evaluating dens fractures, body of C2, & rotary C1-C2 dislocations;
- mach lines - teeth, C1 arch;
- open mouth view, along w/ lateral view, will reveal fractures of the dens ;
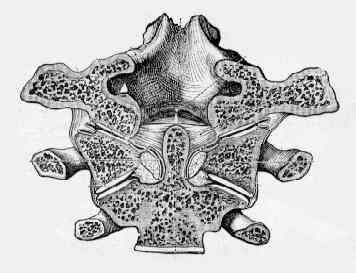
- atlantoaxial articulation & integrity of dens and body of C2 are best seen on the odontoid view;
- this is most technically most difficult film to obtain as it requires patient to open his mouth as wide as possible;
- lateral masses of C1 should align over the lateral masses of C2;
- lateral displacement of masses of C1 w/ respect to C2 may indicate Jefferson or burst fracture of the Atlas;
- combined lateral mass displacement > 7 mm suggests that transverse ligament is torn;
- children:
- overlapping lateral masses can be a normal variant in children and therefore this view may not allos assessment of whether frx is
stable or unstable;
- Normal Variants of Dens: (see dens frx)
- dens may be completely absent, hypoplastic, or incompletely fused to body of C2 (lesion called Os Odontoideum)
- Os Odontoideum is smaller than normal dens & is fixed to anterior ring of C1: 2 move as a unit;
- subluxation and instability are common;
- Assessment of RA Patient:
- state of the odontoid peg and the lateral processes can be assessed by open mouth views, though disease of the tempomandibular
joint can make this difficult;
- concomitant vertical subluxation may conceal amount of anteroposterior movement at the atlantoaxial level because broader base of
odontoid peg comes to lie opposite anterior arch of the Atlas;
- Technique:
- the patient is positioned as for the supine AP;
- central beam directed perpendicular to the midpoint of the open mouth;
- patient should softly say 'ah' to depress the tongue to the floor of mouth during exposure
- Normal Case Examples:

