

- Discussion:
- most common type seen in children & young adults;
- occurs in about 5% of the population;
- more common in Eskimos;
- more common in yound white males involved in hyperextension activities;
- most common at ages 5-8 years;
- results from shear stress at pars intra-articularis, and is more common in repetitive hyperextension activities;
- associated conditions:
- spina bifida occulta;
- those w/ more severe degrees of slipping early in life are most oftenfemale, and it is most often associated w/ Spina Bifida
occulta and L5 to S1;
- thoracic kyphosis;
- Scheuermann's disease;
- Clinical Manifestations:
- usually at L5-S1, usually presents w/ back pain (instability), deformities
or alteration in gait "pelvic waddle" & hamstring spasm;
- Kyphosis of lumbosacral junction w/ or w/o palpable step off;
- severe slips may be assoc w/ radicular findings (L5);
- this occurs from compression between the superior end plate of the caudad vertebrae and the inferior facet of the cephalad vertebrae
- Radiographs: 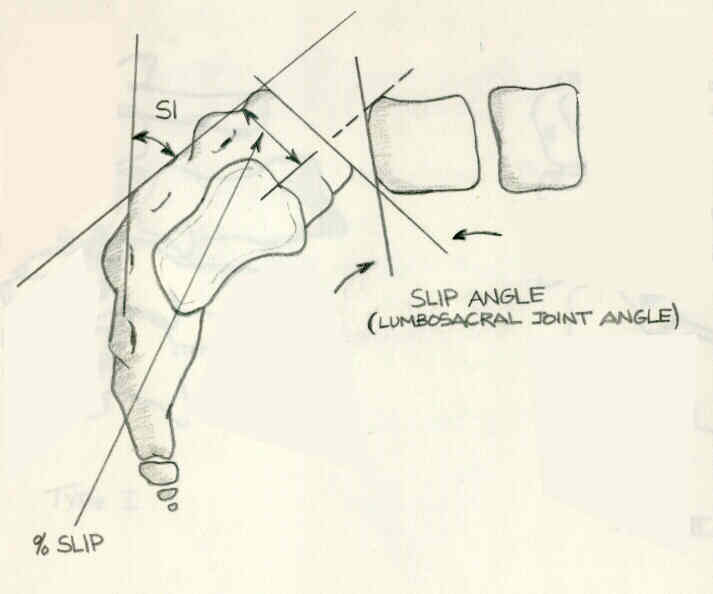
- Grade I:
- Grade II:
- Grade III and IV:
- Treatment:
- although most patients will develop isthmic spondylolithesis in childhood and adolescence, most patients (90%) who require
surgery are adults;
- treatment is based on grade (I, II, III and IV) and clinical findings;
- w/ high grade L5-S1 slip consider additional fusion to L4-5 (especially if MRI shows L4-L5 disc degeneration);
- wide neuroforaminal decompression is also usually required;
- Gill Procedure:
- of historical interest;
- involves removal of the loosely attached arch of L5;
- procedure was complicated by recurrence of pain and progression of deformity