

- See:
- Axis:
- Hyperextension Injury
- Discussion:
- frx of pars interarticularis of C2 & disruption of C2-C3 junction
- type of traumatic spondylolisthesis - "Hangman's frx"
- term "hangman's fracture" is not accurate for the majority of cases, because mechanism of injury for clinically encountered frxs often
lacks large traction force present in judicial hangings;
- in cases in which there is neurologic injury, there will usually be significant horizontal translation w/ accompanying damage to the
posterior longitudinal ligament w/ or w/o damage of the C2-C3 interspace;
- mechanism of injury in adults:
- judical lesion: hyperextension and distraction;
- hyperextension w/ vertical compression of posterior column, & translation of C2 and C3;
- forceful extension of already extended neck is most commonly described mech of injury, but other causes include flexion of flexed
neck & compression of an extended neck;
- a blow on the forehead forcing the neck into extension is a classic mechanism of injury producing fractures thru the pedicles of C2
known as traumatic spondyloslisthesis of C2;
- children:
- injury involves a combination of flexion and distraction;
- injury is rare in children less than 8 years of age, since most fractures will occur thru the odontoid synchondrosis which does not
fuse until age 6-7 yrs (see development of dens and pediatric dens frx);
- Radiographs:
- Cross Table Lateral (injury is readily seen on x-ray)
- Levine Classification: (does not apply to children);
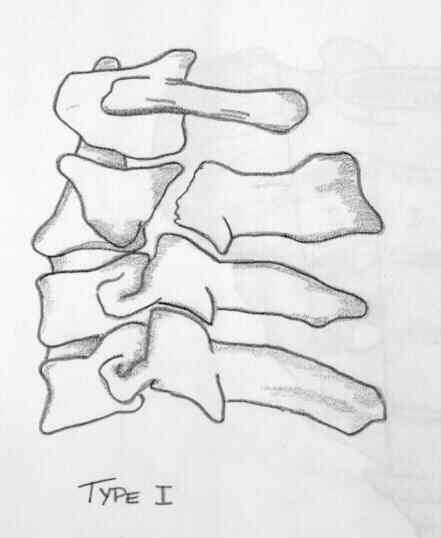
- Type I:
- < 3 mm translation, no angulation;
- bilateral pars frx, prevertbral soft tissue swelling, w/ normal disc space & normal alignment;
- C2-3 disk and ligamentous structures remain intact;
- may be treated with a cervicothoracic brace (SOMI) which limitis flexion
- type I A:
- minimal translation and little or no angulation;
- CT demonstrates extension of fracture through the foramen transversum (which may injure the vertebral artery);
- Type II: 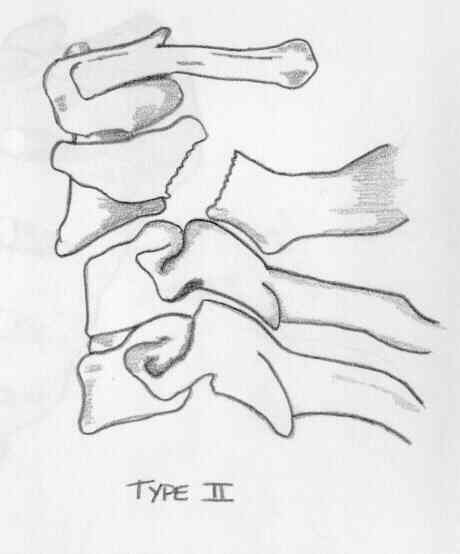
- most common fracture subtype;
- greater than 3 mm translation, and greater than than 10 deg angulation;
- these frx are apparently caused by hyperflexion and are unstable;
- frx is manifested by pars frx, anterior displacement of C2 body, & disruption & asymmetric widening of C2-3 disc
space as well as soft tissue swelling;
- C2-3 disk and posterior longitudinal ligament are disrupted;
- anterior longitudinal ligament usually remains intact;
- type II is typically rx'ed w/ halo vest for 3 months;
- type II injuries may be difficult to manage;
- following reduction, halovest trial is reasonable, but this device may not maintain alignment.
- type IIa:
- flexion/distraction variant, unstable;
- fracture line is more oblique than vertical and there is more angulation vs translation;
- posterior C2-3 disc space widening (more w/ traction);
- type IIA, in addition to frx of type II, has widening of posterior part of C2-3 disk w/ traction, & should be rx'ed in halovest;
- this is also rx'ed w/ halo vest, but avoid overdistraction;
- halo traction may cause overdistraction of this frx;
- traction may cause further fracture displacement and is avoided;
- Type III:
- includes all characteristics of type II frx as well as bilateral interfacetal dislocation;
- may require open reduction of facet dislocation halo immobilization for the pedicle injury;
- type III has angulation, translation, and also unilateral or bilateral facet dislocation at C2-3.
- Non Operative Rx:
- halovest
- pts w/ Hangman's fx should not be placed in cervical traction if mechanism of injury involves extension or distraction;
- children:
- traction should generally be avoided;
- reduction is obtained w/ gentle extension;
- some residual displacement may be accepted;
- need to immobilize in halo for 6-8 weeks;
- Surgical Treatment:
- ORIF may be necessary to obtain and maintain reduction;
- internal fixation techniques include posterior oblique wiring, which resists rotational forces, & screw fixation of C-2 posterior elements
to the C-2 body.
- this latter technique depends on integrity of C-2 & C-3 capsules and ligaments, which is usually the case.
Injuries of the atlas and axis. A follow-up study of 85 axis and 10 atlas fractures.
Fractures of the neural arch of the axis. A report of twenty-nine cases.
Caspar plate fixation for the treatment of complex hangman's fractures.
Traumatic spondylolisthesis of the axis.
The management of traumatic spondylolisthesis of the axis.
Axis fractures: a comprehensive review of management and treatment in 107 cases.