


Case Example by James R. Urbaniak MD.
- Discussion:
- regional fasciectomy is the most commonly performed procedure for Dupuytren's contracture;
- current trend is for limited palmar and digital fasciectomy confined to contracted rays;
- in the report by Armstrong JR, et al (2000), the authors reviewed 143 rays in 103 patients undergoing dermofasciectomy for diffuse disease with involvement of the skin;
- there was recurrence in 12 rays (8.4% of rays; 11.6% of patients) during a mean follow-up of 5.8 years;
- ref: Dermofasciectomy in the management of Dupuytren's disease
- Surgical Technique:
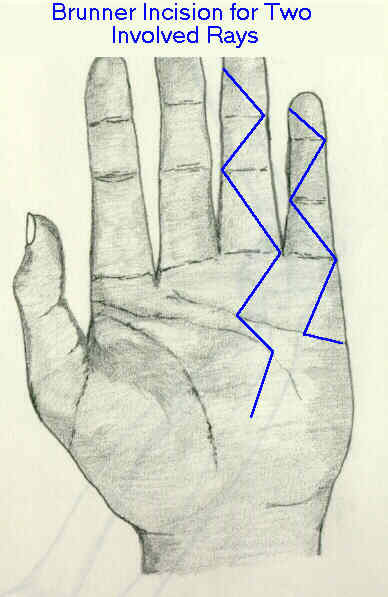
- surgical incision:
- Urbaniak (personal communication) uses a Brunner incision and recommends that the little finger incision cross the phalangeal crease
on the ulnar border (as is seen in the diagram);
- incision is carried down thru the skin, but care is taken to avoid incising too deeply over the MCP joints (since the N/V structures
may lie especially superficial at this location);
- always consider the quality of the skin and position of the cords before making incisions;
- obviously it would not be wise to have the base of a flap underneath a thickened cord which is densely adherent to the skin since this
could potentially devascularize the entire flap when the cord is removed;
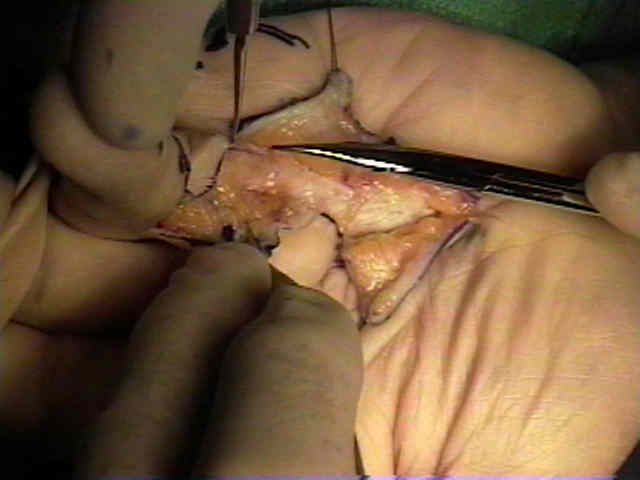
- pre-tendinous cords
- proximal to the metacarpal heads, the knife can be used to elevate the skin and the subcutaneous tissues off the palmar fascia and pretendinous cords;
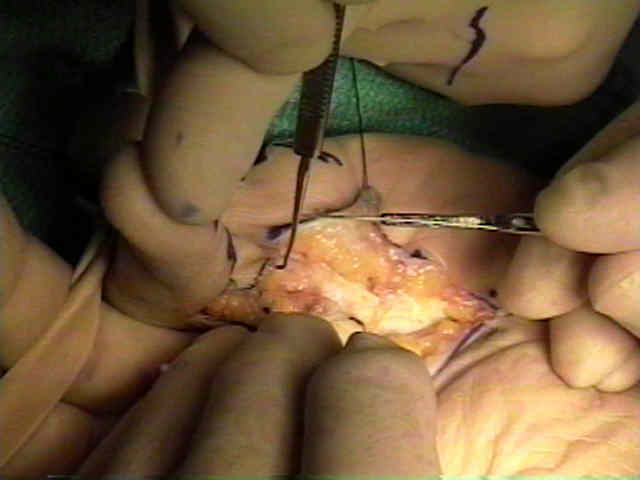
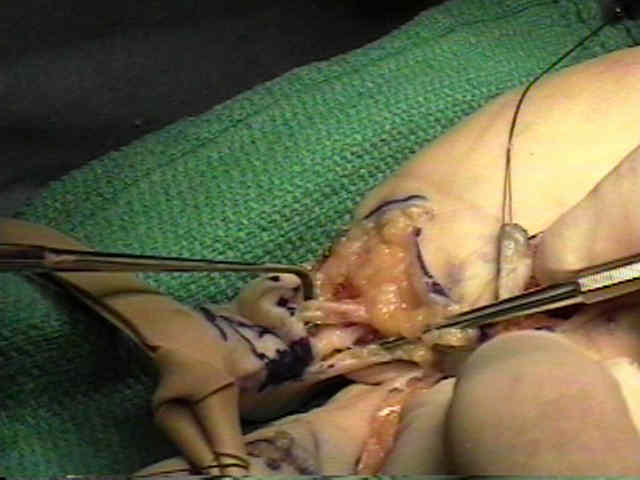
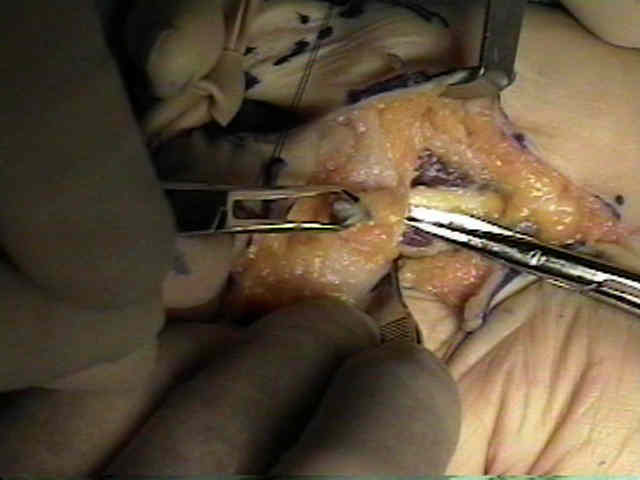
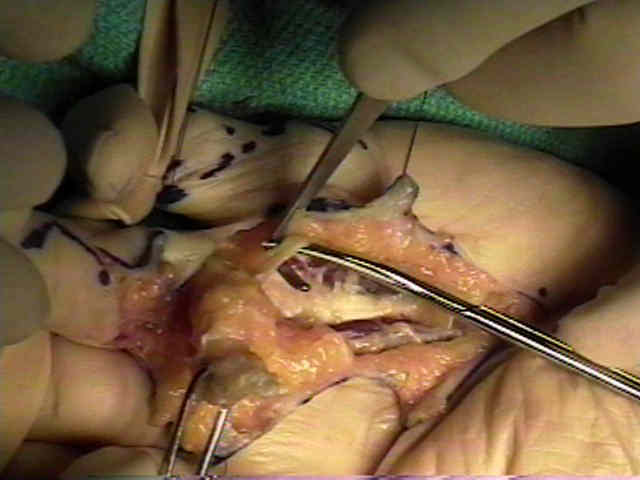
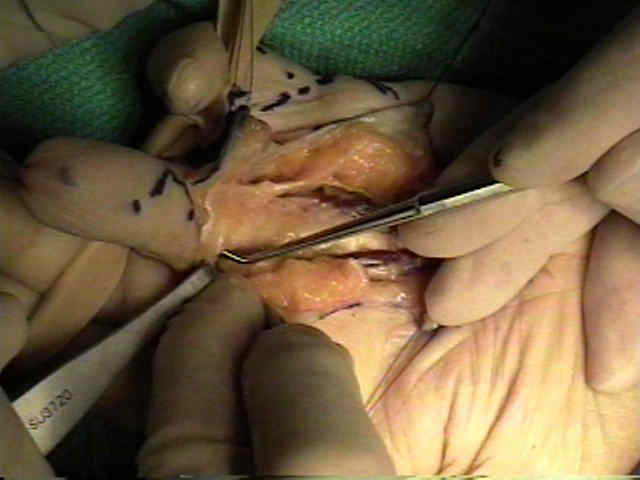
- identification of nerves and vessels:
- over the metacarpal heads, tenotomy scissors are used to spread thru the subcutaneous tissues until both digital nerves and arteries are identified on each side of the cord;

- spiral cord:
- recognize that the sprial cord may pass underneath the N/V structures, which causes them to shift centrally and superficially;
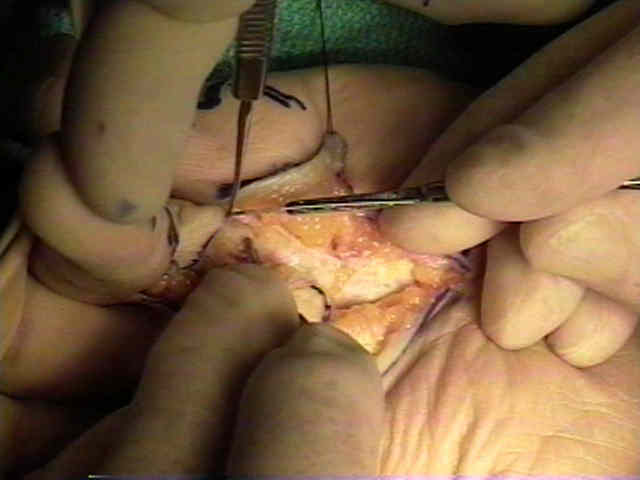
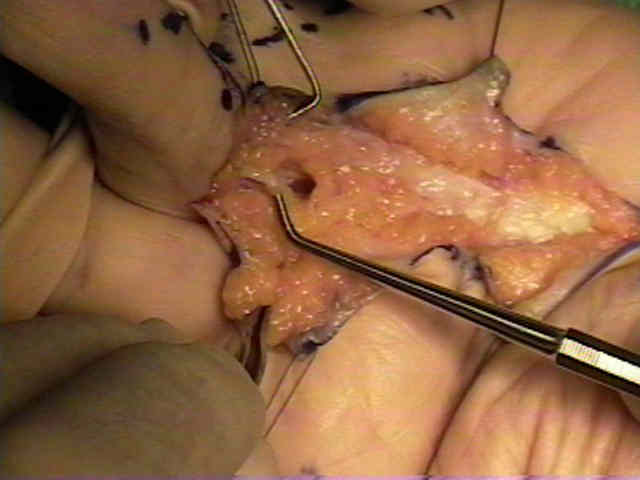
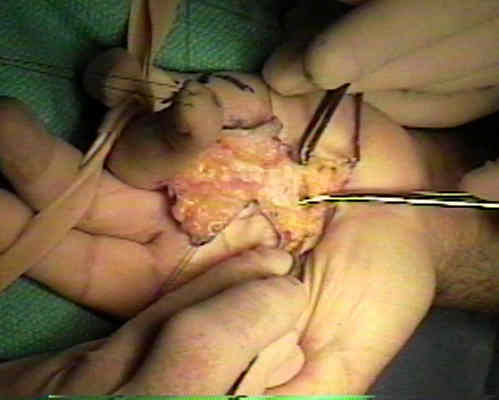
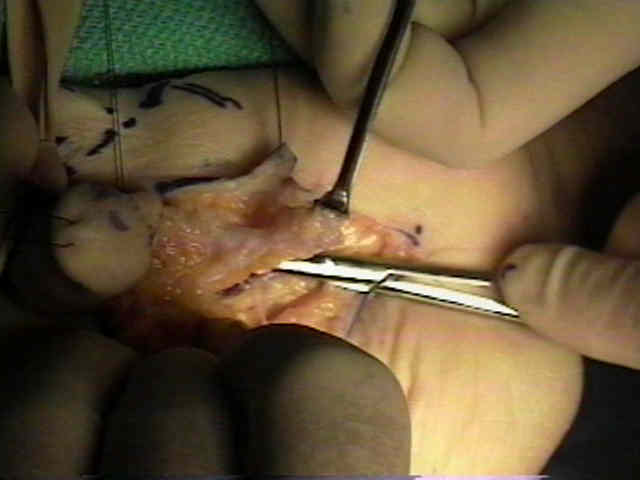
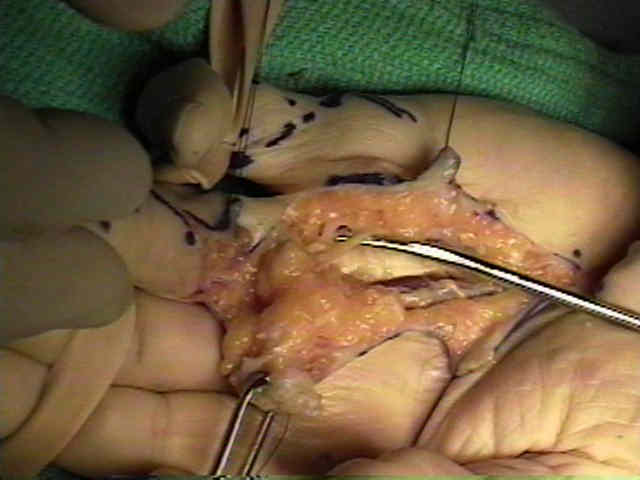
- regional fasciectomy:
- once the digital nerves and vessels have been identified, a beaver blade is used to fashion a distally based trap door of diseased palmar fascia;
- the proximal edge of the flap is grapsed w/ a clamp and is elevated inorder to provide tension;
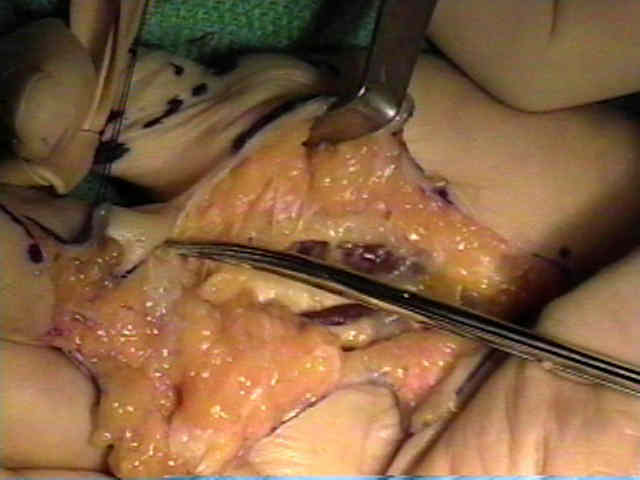
- this thickend fascia is progressively elevated and dissected distally;
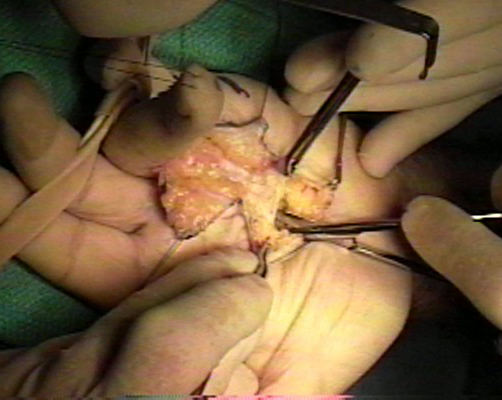
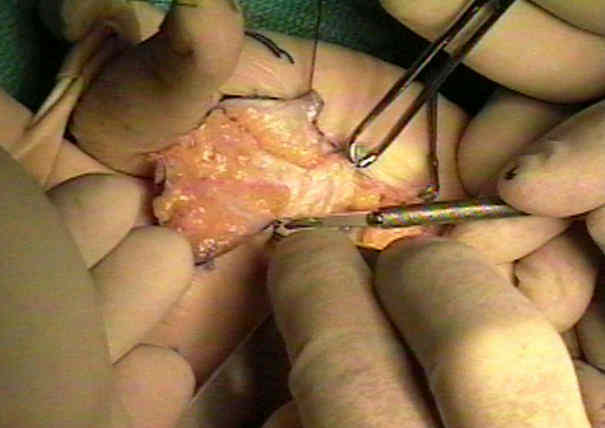



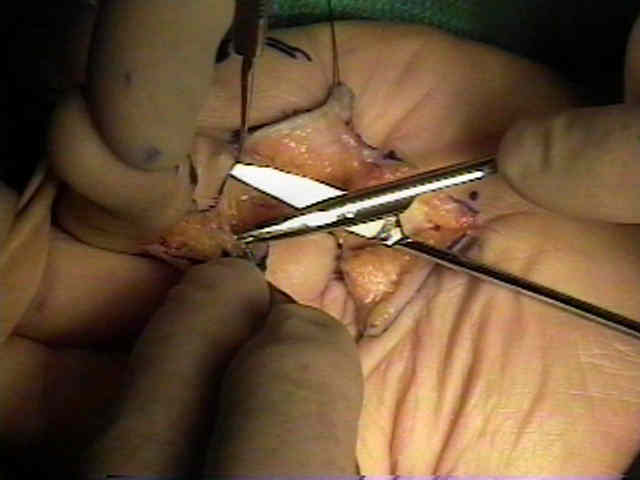
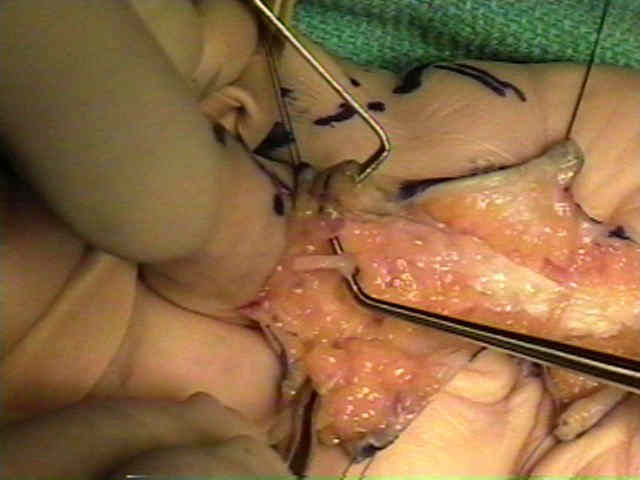
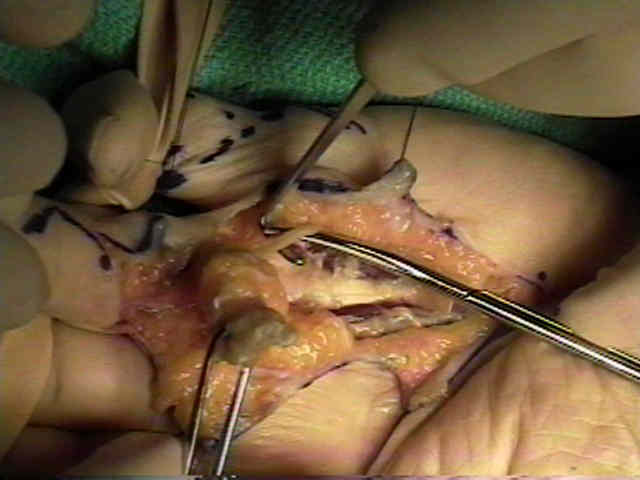
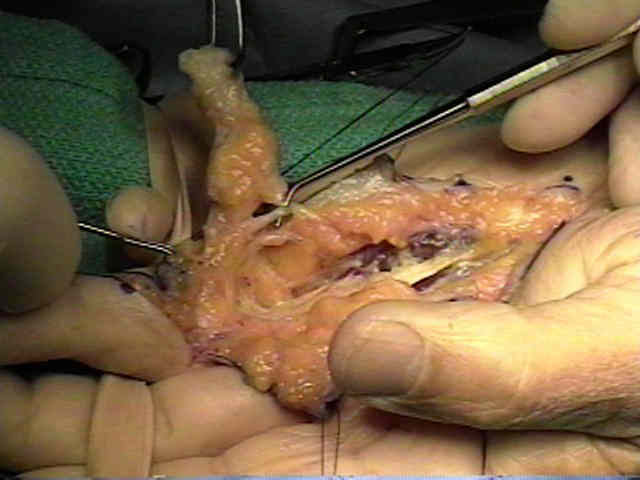
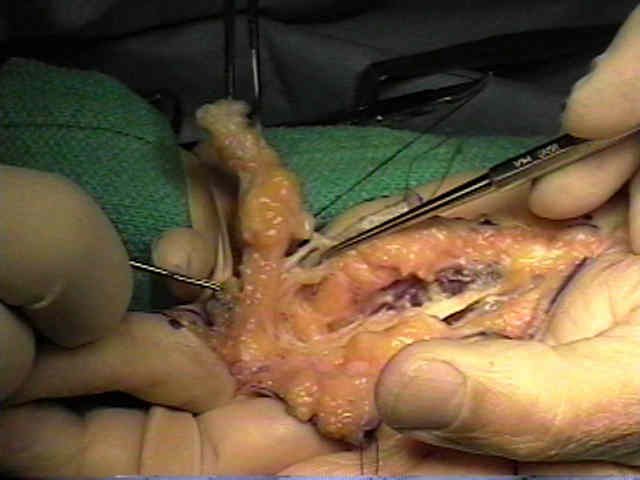
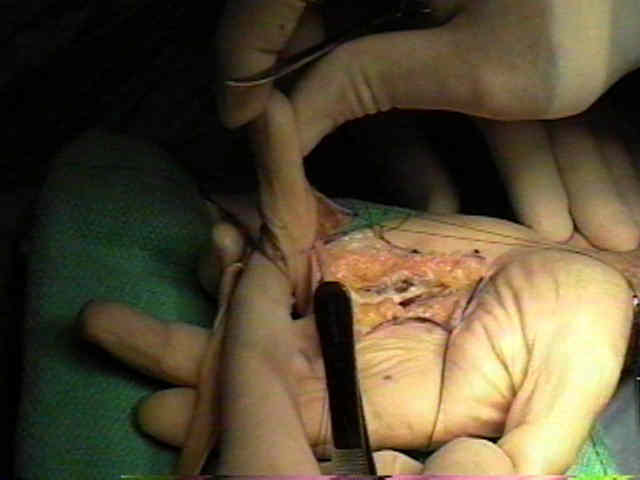
- once the dissection reaches the metacarpal heads great care is taken to carefully dissect the digital nerves and vessels off the diseased palmar fascia;
- as Urbaniak points out, usually one digital vessel will be more encased in thickened fascia than the other;
- if possible attempt to leave one vessel undisturbed in its bed of areolar tissue (which avoids possibility of arterial spasm);
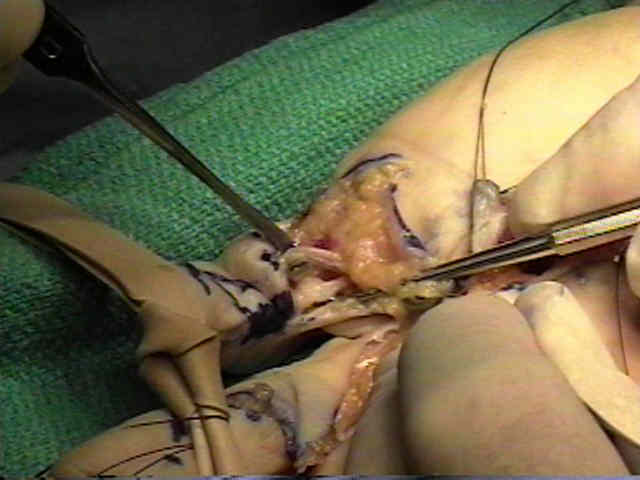
- once the digital nerve and vessel are freed, the fascial cord is excised;
- Post Op:
- carefully fashioned bulky hand dressing is manditory;
- some advocate several days of immobilization of hand w/ slight wrist extension along w/ MP flexion and slight PIP flexion before early mobilization is started;
- it is essential to avoid postoperative stiffness;
- pain in the post operative period must alert the surgeon of possible post operative hematoma;
- Complications:
- post operative complications include recurrence hematoma, skin loss, infection (treated with early debridment), joint stiffness, and occassionally RSD;
- use of K wires is thought to promote infection
Treatment of Dupuytren's contracture. Long-term results after fasciotomy and fascial excision.
Segmental aponeurectomy for Dupuytren's disease: a prospective study
Segmental aponeurectomy in Dupuytren's disease.
Treatment of Dupuytren's contracture. Long-term results after fasciotomy and fascial excision.
Fasciotomy and Z-plasty in the management of Dupuytren's contracture.