

- Discussion:
- two sites have been proposed for nail entry:
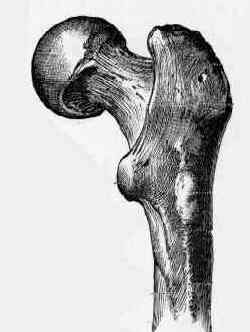
- tip of the greater trochanter and the piriformis fossa;
- Entry thru Piriformis Fossa;
- main advantage a colinear trajectory with the long axis of the femoral shaft
- accurate positioning of the entrace hole is critical.
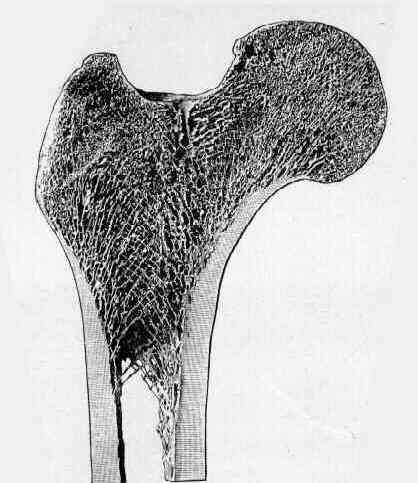
- anterior bow of shaft curves up to posterior tip of greater trochanter;
- beginning awl should be inserted:
- just posterior to midline of trochanter;
- just medial to prominence of trochanter in trochanteric fossa.
- when an IM guide wire is passed in retrograde manner in cadaver femora, entry point is slightly anterior in piriformis fossa;
- however, entrance portal anterior to the midpoint of the trochanter may result in perforation of the anterior cortex of the proximal femur;
- entry that is too far anterior results in deformation of nail & comminution of the proximal fragment;
- entry that is too far medial, may result in femoral neck fracture;
- for nails that are designed for piriformis entry, lateral placement throught the trochanter may cause varus alignment of proximal fractures;
- entry in posterior aspect of piriformis fossa generates least stress in femur;
- such placement ensures that hole will be aligned w/ longitudinal axis of medullary canal in both sagital & coronal plane;
- excessive medial placement:
- may create a stress riser in femoral neck;
- may also comprimise the vascularity of the femoral head;
- disadvantages:
- peritrochanteric pain;
- end branches of the medial femoral circumflex artery cross near this point;
- in the report by Dora, et al, nailing with a reamed AO universal femoral nail was performed on 16 adult cadavers
followed by dissection of the proximal part of the femur to assess possible damage to the soft tissues;
- 3 entry portals were defined;
- entry portal lateral to the junction of the neck and the greater trochanter;
- partial avulsion of the piriformis and the obturator internus tendon were present in four and in one of five specimens;
- entry portal at the base of the greater trochanter anterior to a line along the longitudinal axis of the femoral neck;
- showed injuries to the piriformis tendon in two and to the gluteus minimus tendon in one of four cases;
- entry portal at the base of the greater trochanter posterior to a line along the axis of the femoral neck (at the piriformis fossa).
- partial avulsion of piriformis, obturator internus, and obturator externus were encountered in five, six, and 2/7 specimens;
- anterior branches of the ramus profundus of the m.f.c.a. within the synovial fold were damaged in all of these cases;
- results of the current study favor the nail entry portal lateral at the greater trochanter;
- ref: Entry Point Soft Tissue Damage in Antegrade Femoral Nailing: a Cadaver Study
- Entry through Greater Trochanter:
- may avoid damaging blood supply to the femoral head and resultant AVN, femoral neck frx, and septic arthritis;
- entry through greater troch will lead to eccentric reaming from lateral to medial, which may lead to comminution of medial cortex
of proximal fragment and varus deformity of proximal fragment;
- laterally placed portal at tip of trochanter may lead to eccentric reaming and medial comminution of the proximal fragment;
- this will comprimise the interlocking of the proximal screw;
- proper starting point for trochanteric nails, is just lateral to the trochanteric axis;
- iatrogenic segmental splitting of greater trochanter may occur in 5% of patients, and femoral neck fracture in 3% of patients;
- varus malalignment of the fracture, esp in proximal shaft fractures nailed w/ patient in a supine position, may be complication of
entrance hole placed in trochanteric tip. (i.e., lateral placement of entrance hole)
- Misc:
- if the starting point needs to be medialized (as with subtrochanteric fractures), use a rongeur remove medial bone to
the anterolateral piriformis fossa to avoid varus malreduction with passage of the nail
Curvature of the femur and the proximal entry point for an intramedullary rod.
The effect of the entry hole for an intramedullary nail on the strength of the proximal femur.
Entry point soft tissue damage in antegrade femoral nailing: a cadaver study.
Risk of Superior Gluteal Nerve and Gluteus Medius Muscle Injury During Femoral Nail Insertion.
Functional outcome following intramedullary nailing of the femur: a prospective randomized comparison of piriformis fossa and greater trochanteric entry portals.
An anatomical study of the entry point in the greater trochanter for intramedullary nailing
.........................................................................................................................................................................................................................................................................................................................................