

- See: Ilizarov Technique
- Discussion:
- advantages:
- allows arthrodesis in presence of active infection;
- external fixation is adjustable;
- allows access to the soft tissues;
- leaves no longstanding foreign body;
- requires little additional soft-tissue dissection;
- disadvantages:
- non-rigid fixation;
- potential cause of neurovascular injury;
- requires second procedure for removal of fixator;
- outcomes:
- in the report by Manzotti et al, the authors followed 6 patients (4 women, 2 men) treated between 1992 and 1998;
- average age was 56.6 years (range, 23-70 years) and the mean number of previous surgical procedures was seven (range, 4-10 procedures);
- average followup was 34 months;
- 5 patients who had completed treatment;
- all had obtained a stable knee arthrodesis after a mean external fixation time of 6.8 months without additional surgical procedures or bracing;
- the authors recommended arthrodesis for patients with extensive bone loss, significant limb shortening or axial deformity or both,
active infection, or previous failed arthrodesis.
- ref: Knee Arthrodesis After Infected Total Knee Arthroplasty Using the Ilizarov Method
- Technique:
- implant removal;
- preparation of the osseous bed;
- preparation of the bone ends should expose vascular bone, provide bone apposition, correct limb alignment, and preserve as much
bone stock as possible;
- when bone cuts are being performed, extramedullary TKR cutting jigs can be used to achieve alignment and bone apposition;
- bone resection should be limited to one to two mm of bone from the femur and tibia;
- proximal part of tibia is be cut 1st to provide cut that is 90 deg to coronal plane and has the desired degree of posterior slope in the
sagittal plane;
- limb is aligned in 0 to 5 degrees of valgus, and the distal part of femur is cut parallel to the cut tibial surface;
- bone ends should be vascular, stable, apposed, & in correct flexion and valgus;
- application of the external fixator;
- most external fixators are weak in anteroposterior bending;
- addition of an anterior frame with half-pins improves fixation;
- for knee arthrodesis, a biplanar Ex Fix w/ sagittal pins and a ventral frame to control anteroposterior bending forces provides
improved fixation;
- femoral pins:
- 3 centrally threaded 5 mm transfixing pins are placed in distal part of the femur from medial to lateral, w/femoral vessels being
avoided;
- two anterior half-pins are placed in distal part of femur & two are placed in the proximal part of the tibia and connected to the
frame;
- increased stability is achieved by placing the anterior pins as far as possible from the arthrodesis site;
- bone-grafting;
- bone graft is placed about the periphery of the arthrodesis site to allow revascularization from the surrounding soft tissues;
- posterior bone graft should be placed before the external fixator is tightened;
- Post Op:
- external fixation is maintained until clinical union of arthrodesis site has been achieved, usually at ten to twelve weeks;
- after external fixator has been removed, a cylinder cast is used for four to twelve weeks or until radiographic union is present
- Example using Ilizarov:


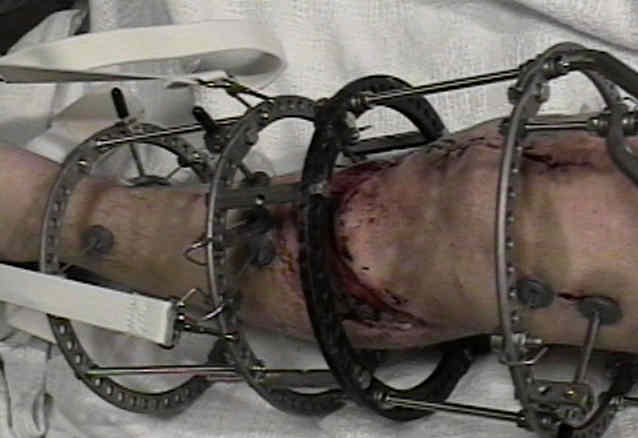


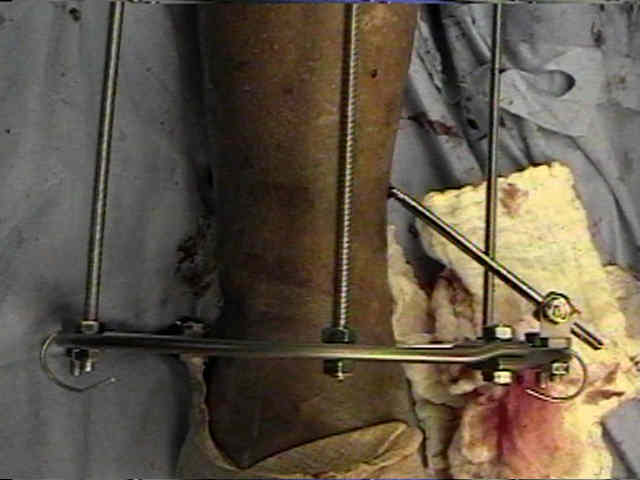
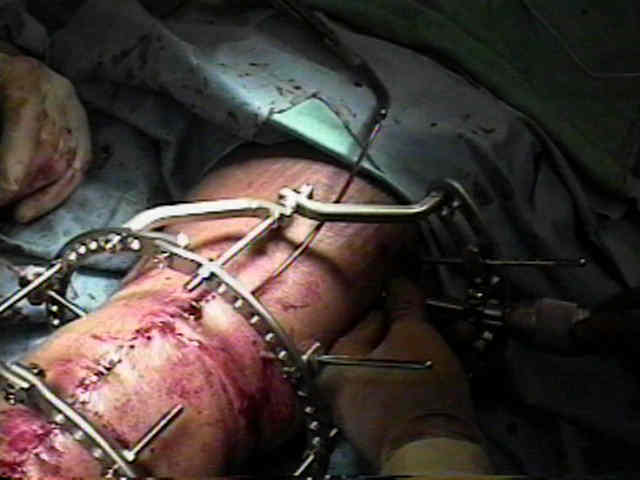
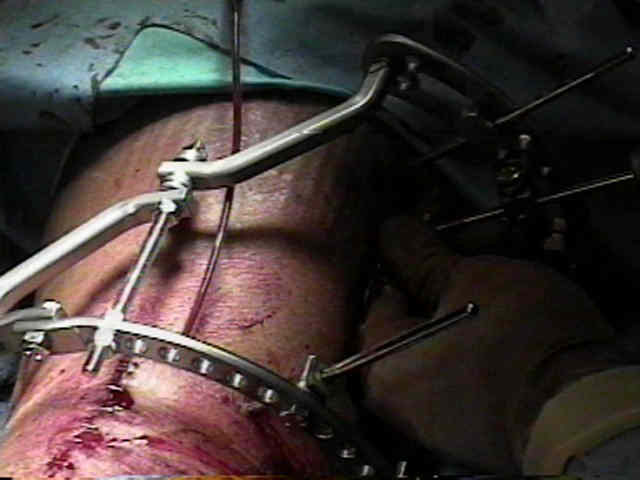

Failed total knee arthroplasty treated by arthrodesis of the knee using the Ace-Fischer apparatus.
Single plane and biplane external fixators for knee arthrodesis.