

- Associated Transverse & Posterior Wall Fracture
- T Shaped Fractures
- AO Foundation Transverse Fracture
- Discussion:
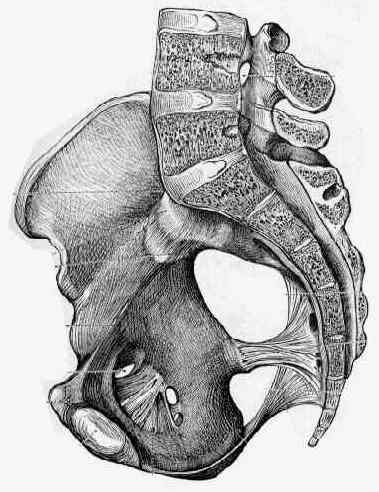
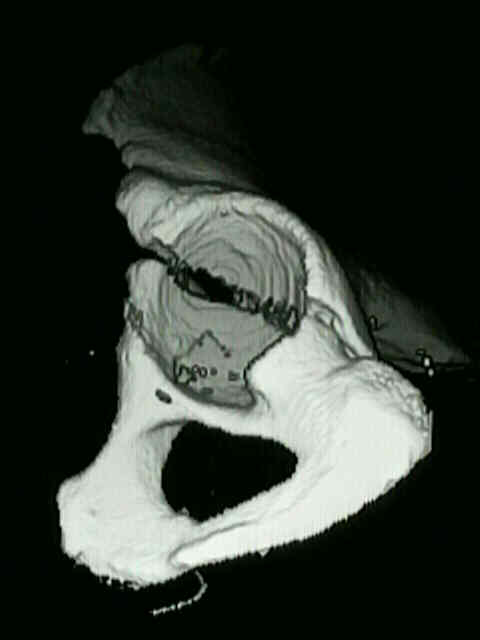
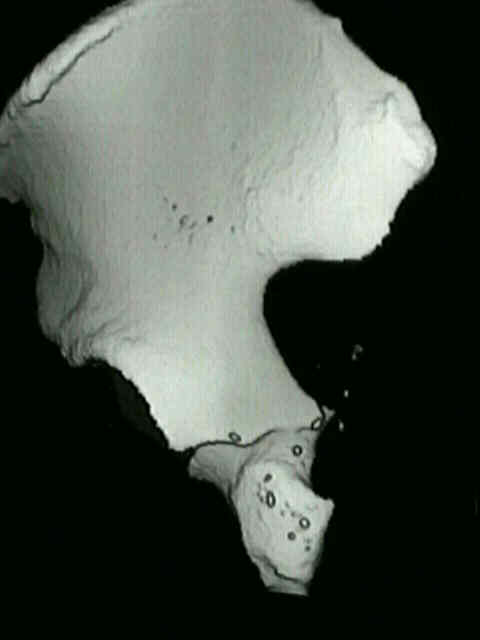
- transverse frxs extend across both the anterior and posterior columns;
- frx divides the innominate bone into superior segment containing acetabular
roof and intact ilium, & inferior segment consisting of single ischiopubic
fragment;
- classification:
- if both anterior & posterior columns are broken, then it is 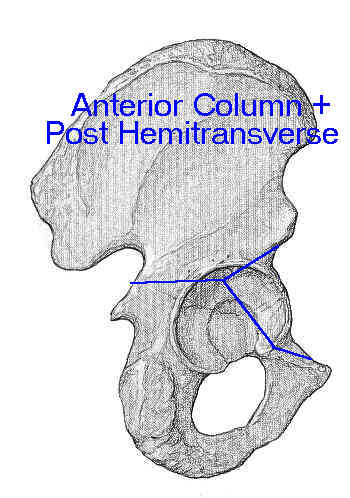 called transverse fracture, and if both
called transverse fracture, and if both
columns are broken & separated from each other, that is T fracture;
- transverse fracture are sub-classified according to location relative to the wt bearing dome;
- transtectal: fracture courses through the weight-bearing dome (WBD);
- juxtatectal: fracture courses above the cotyloid fossa, so that a significant portion of the wt
bearing dome is left intact;
- infratectal: fracture courses below the wt bearing dome;
- transverse posterior wall fracture:
- may be difficult to reduce in the presence of a transverse transtectal component, large posterior
wall fragment, or w/ pubic ramus fracture;
- mechanism: blow directly upon greater trochanter;
- stemming from the lateral compressive force these fracture may also be assoc
w/ central femoral head dislocation;
- Radiographs:
- ilioischial and iliopectineal lines are both disrupted, but there will be no involvement of the obturator
ring (otherwise fracture would be a T fracture);
- assesment of stability:
- in the study by Vrahas, et al 1999, a cadaveric biomechanical study was performed to determine the relative stability
of anterior column, posterior column, and transverse fractures;
- they noted that transverse acetabular fractures with medial roof-arc angle (AP radiograph) of 45 degrees or less were
unstable and required ORIF;
- ref: The effects of simulated transverse, anterior column, and posterior column fractures of the acetabulum on the stability of the hip joint.





- Exposure:
- Kocher-Langenback:
- most transverse frx are exposed w/ posterior approach, especially if the displacement and rotation is posterior;
- transverse frx, posterior wall & posterior column fractures, & T-type fractures may be exposed using Kocher-Langenback;
- in many cases a trochanteric osteotomy will be required inorder to optimize the exposure;
- references:
- Quality of radiographic reduction and perioperative complications for transverse acetabular fractures treated by the Kocher-Langenbeck approach: prone versus lateral position.
- Treatment of Transverse with or without Posterior Wall Fractures of Acetabulum Using a Modified Smith-Petersen Combined with Kocher-Langenbeck Approach.
- ilioinguinal approach:
- indicated for high transverse frx and for frx w/ anterior displacment and/or w/ anterior rotation;
- ilioinguinal approach should also be chosen for transverse fractures which course across the acetabulum from a proximal-
anterior to a distal-posterior direction;
- ref: Patients undergoing surgical hip dislocation for the treatment of acetabular fractures show favourable long-term outcome.
- Reduction:
- for reduction of these frx pt is generally prone & Kocher Langenbeck approach is used;
- reduction technqiue is similar to that used for posterior column frx;
- usually the two screw technique is used to control displacement while rotational lever is placed to control the ischial tuberosity;
- as rotational lever is being applied, the entire ischiopubic segment is rotated rather than the posterior column alone;
- reduction of anterior portion of transverse frx is assessed by palpation of quadrilateral surface & pelvic brim thru greater sciatic notch;
- insertion of Schanz screw:
- w/ the posterior approach, reduction can be facilitated by inserting a Schanz screw into the ischium just inferior to the
subcotyloid gutter;
- T chuck is applied over the the Schanz screw, which is then used to rotate a displaced posterior column frx into
a reduced position;
- surgeon's other hand can guide the reduction by palpating the quadrilateral surface;
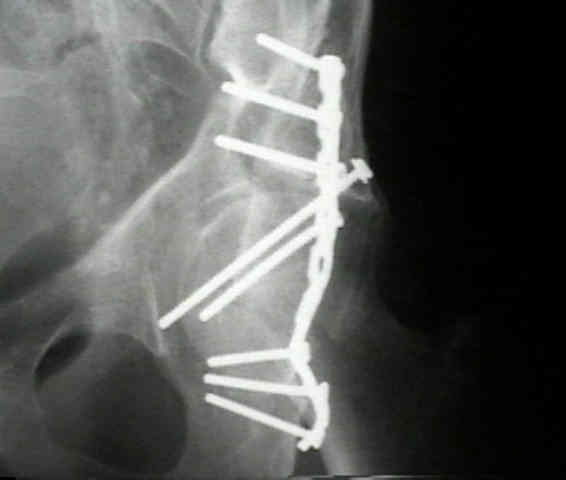
- Fixation:
- lag screw spans transverse frx from a proximal to a distal direction;
- long 6.5 mm cancellous screw transverses the anterior portion of frx into the superior pubic ramus;
- lag screw is inserted into retroacetabular surface and is directed toward the anterior column;
- following lag screw, a plate is placed along retroacetabular surface;
- plate fixation:
- 3.5 mm reconstruction plate is applied along posterior column, immediately behind the acetabulum;
- in the report by Chang et al, the authors evaluated the strength of lag screw fixation compared with traditional fixation techniques
of transverse acetabular frx;
- 10 cadaveric pelvic specimens with bilateral, transtectal transverse acetabular fractures were used for this study;
- right acetabular fractures were fixed with a 5-hole plate and four screws with the central hole spanning posterior fracture site;
- left acetabular fractures were fixed w/ 2 lag screws, 1 each in the anterior and posterior columns, or with a screw and wire
construct stabilizing both columns;
- plate and screw construct showed significantly greater yield and maximum strength when compared with the two lag screws;
- stiffness of lag screw method was 39% higher than that of the plating method, but this result was not statistically significant;
- ref: Comparative Strength of Three Methods of Fixation of Transverse Acetabular Fractures
- Screw Placement in the Ischial Tuberosity:
- anatomical hazards:
- the internal pudendal bundle usually lies 1.5 cm from the medial posterior margin of the ischial tuberosity;
- internal pudendal bundle passes out of greater sciatic foramen, passes around sacrospinous ligament, over internal obturator
muscle (just medial to tuberosity) and then into lesser foramen;
- excessively medially angulated screws may injure the internal pudendal;
- at 2 cm below inferior acetabular margin, hamstring origin is encountered (and therefore dissection below this point is avoided);
- technique of insertion:
- maximal purchase is achieved w/ entry into the tuberosity 5 or 10 mm medial to the lateral margin of the tuberosity and are
directed inferiorly;
- at the level of the inferior acetabular margin, direct the screw 35-40 deg caudally;
- at 1 cm below the inferior acetabular margin, direct screws 45-50 deg caudally;
- at 2 cm below the inferior acetabular margin, direct screws 50-55 deg caudally

The Effects of Simulated Transverse, Anterior Column, and Posterior Column Fractures of the Acetabulum on the Stability of the Hip Joint
Results after operative treatment of transverse acetabular fractures.
Operative treatment of transverse acetabular fractures: is it really necessary to fix both columns?
Value of 3-D CT in Classifying Acetabular Fractures During Orthopedic Residency Training
Comparative strength of three methods of fixation of transverse acetabular fractures