- Optimize the Exposure:
- it is important to fully expose the proximal tibial surface inorder to avoid iatrogenic injury to the collateral ligaments, the PCL, or
even the posterior neurovascular structures;
- soft tissue stripping: (see medial and lateral capsular exposure)
- ensure that there has been adequate soft tissue stripping on both the medial and lateral sides of the proximal tibia;
- usually the medial side has already been stripped but often there has been inadequate soft tissue stripping laterally since
visualization is obstructed by the extensor mechanism;
- this stripping helps book the tibia forward, which assists with exposure;
- w/ the patella everted and the knee flexed, the lateral side is opened up and therefore it can be safely stripped w/ a knife and an osteotome;
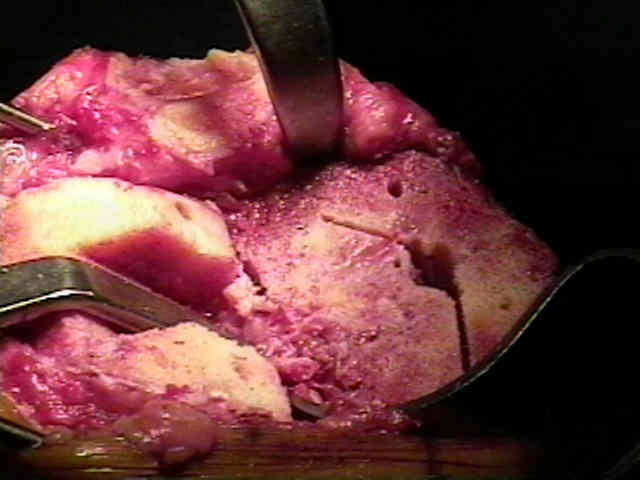
- resect remnant menisci:
- this should be performed prior to the proximal tibial cut since it improves visualization;
- it is important to sharply remove the remaining menisci, but beaware of the potential for vascular injury;
- the popliteal artery lies behind the posterior horn of the lateral mensicus, and will be partially
protected by the popliteus mucle;
- the popliteal vein lies directly posterior;
- menisci are removed by pulling them into the joint and transecting them w/ the knife blade directed parallel to posterior tibial surface;
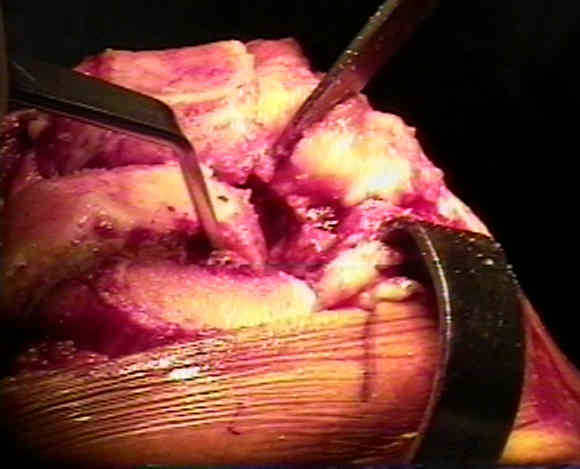
- apply retractors:
- curved knee retractors are applied to both the medial and lateral sides of the joint;
- lateral retractor needs to be placed slightly anterior to the midcoronal plane inorder to better protect patellar ligament during proximal tibial cut;
- curved "pitch fork" retractor is placed behind the proximal tibia straddling the PCL;
- use the pitch fork retractor to gently lever the tibia forward, which places the PCL under tension;
- often the pitch fork is required to lever the tibia forward, so that exposure of the posterior tibial plateau is achieved;
- cruciate ligaments:
- if PCL retaining prosthesis is to be used, then carefully use cautery to elevate
ACL and the most anterior portion of the PCL of the super surface of the tibia;
- if a posteror stabilized prosthesis is to be used, the PCL will already have been removed by the box cuts;
- this step will allow the tibia to be translated anteriorly, which both improves visualization of the posterior tibial
surface and moves the tibia further away from the posterior neurovascular structures;
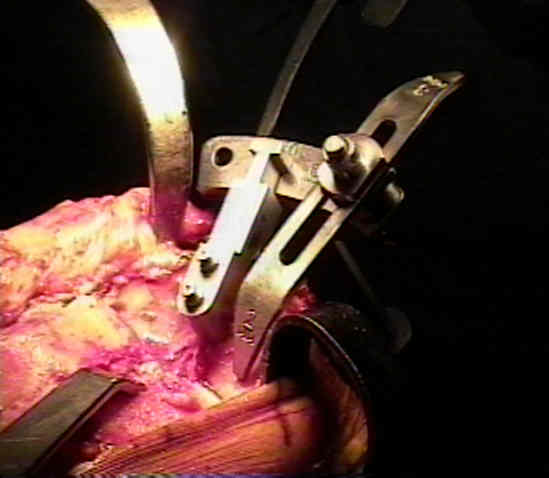
- Tibial Cutting Guides:
- intra-medullary alignment guide:
- in the report by MR. Reed et al (JBJS-Br. Vol 84-B Number 6 August 2002), the authors undertook a prospective, randomised
study of 135 TKR to determine the most accurate and reliable technique for alignment of the tibial prosthesis;
- tibial resection was guided by either intramedullary or extramedullary alignment jigs;
- correct tibial alignment was found in 85% of the intramedullary group compared with 65% of the extramedullary group (p = 0.019);
- the authors concluded that IM guides are superior to extramedullary instruments for alignment of the tibial prosthesis
- tibial extramedullary guide