

- see:
- tibial component
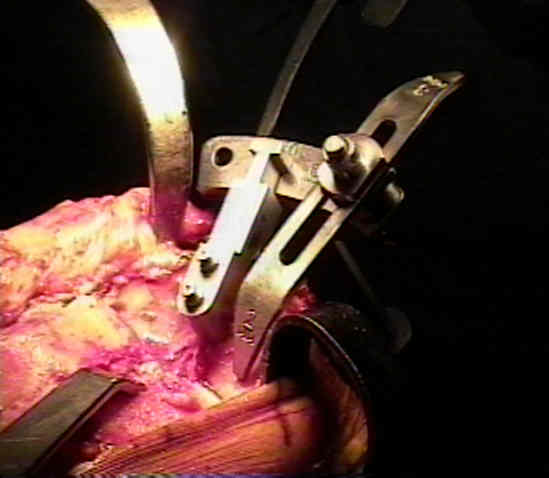
- extra-medullary cutting guide;
- preparation for proximal tibial cut
- posterior slope
- this cut is made at right angles to anatomical axis of tibia;
- proximal tibial cut is made 2 mm below the anterior surface of the more involved side;
- in knee with fixed varus deformity more bone is resected from lateral tibial plateau than off the medial tibial plateau;
- alternatively, the resection can be based off the less involved side;
- cut should be < 5 mm below tibial plateau because tibial cancellous bone weakens rapidly as distance from articular surface increases;
- due to complex geometries that may be present on degenerative tibial surface, it may be prudent to "eyeball" depth of proximal cut,
rather than relying on stylus;
- reliance on the stylus alone may result in a inadvertently deep cut on the lesser involved side;
- quick trial:
- if the femoral cuts have already been made (and the femoral trial is in place), insert a trial base plate w/ an 8 mm spacer while
knee is in full extension;
- if the 8 mm spacer cannot be easily inserted (in full extension) then it is unlikely that a 10 or 12 mm spacer will be able to
be inserted (and therefore further proximal tibial resection is required);
- consequences of excessive proximal tibial resection:
- lowering of the joint line;
- loss of bone quality;
- quality of cancellous bone in the tibia is best in immediate subarticular area, and decreases rapidly w/ more distal resection;
- loss of surface area:
- surface area of the proximal tibia decreases w/ more distal cut;
- distal resection jeopardizes attachments of IT band & pes anserinus, MCL and PCL;
- PCL takes origin from posterior aspect of proximal tibia, so that its attachment is not lost when proximal tibia is resected
just below the articular surface;
- valgus instability may result from an excessively deep resection along w/ an excessively steep posterior slope (the later may
remove the posterior oblique ligament;
- resection more than 1 cm below original articular surface:
- cuts at this depth require bone grafts or revision components;
- due to loss of PCL, a posterior stabilized prosthesis: will be required;
- in presence of severe deformity, proximal tip of fibula, normally located approx 1 cm below tibial articular surface, is good
guide for the level of maximum resection
Analysis of the bone surface area in resected tibia. Implications in tibial component subsidence and fixation.
How much tibial resection is required in total knee arthroplasty?