- Discussion: (w/ assistance and narration by Dr Kyle Dickson MD)
- term pilon (hammer) fracture was introduced to describe these compression injuries by Destot in 1911;
- ref: High-energy tibial pilon fractures: an instructional review.
- frx components:
- combination of ankle frx & distal tibial metaphyseal frx, usually w/ intra articular comminution;
- frx of medial malleolus;
- frx of anterior margin of tibia;
- transverse frx of posterior tibial surface;
- 20-25% of these will be open;
- mechanism of injury:
- vertical loading drives talus into distal tibia;
- position of foot & rate of loading affect injury pattern;
- it is important to distinguish between low energy frx (from skiing) vs high energy frx (as from MVA);
- plantar flexion: posterior articular damage;
- dorsiflexion: anterior articular damage;
- fibular frx:
- if fibula is frxed, then force involved is usually valgus shear w/ severe injury to the lateral aspect of the joint;
- fibula intact: (25% of injuries);
- pilon frx w/o assoc frx of fibula occur in approx 15 % of cases;
- w/ compression injuries fibula may remain intact, which never happens w/ shearing type injury;
- w/ intact fibula, ankle is often driven into varus w/ severe impaction of the medial part of the tibial plafond;
- associated injuries: (30% will have ipsilateral injuries and 5-10% will have bilateral injuries;)
- compartment syndrome
- Acute compartment syndrome of the foot following fixation of a pilon variant ankle fracture
- compression frx of vertebral column, particularly L1;
- contralateral fractures of: os calcis, tibial plateau, pelvis, or acetabulum (verticle shear injuries):
- vascular injuries:
- Vascular abnormalities as assessed with CT angiography in high-energy tibial plafond fractures.
- outomes:
- with operative treatment, high energy pilon fractures will take 4 months on average to heal;
- 75% of patients who do not develop wound complications may expect a good result;
- subsequent arthrodesis rate may be as high as 10%;
- large number of patients will have pain even after 2 years post injury;
- references:
- Tibial Plafond Fractures. How Do These Ankles Function Over Time?
- Outcomes After Treatment of High-Energy Tibial Plafond Fractures.
- Outcome Following Open Reduction and Internal Fixation of Open Pilon Fractures
- The Sequential Recovery of Health Status after Tibial Plafond Fractures
 - Exam:
- Exam:
- soft tissue: note presence of swelling and any fracture blisters;
- perform an Allen test using a pulse oximeter for the foot vasculature (pulse ox is placed on the toe);
- note function of posterior tibial pulse while the dorsalis pedis pulse is occluded and vice versa;
- ideally, the pulse ox should demonstrate normal mp3e forms even w/ occlusion of either vessel;
- reference: The management of the soft tissues in pilon fractures.
- Radiographs: 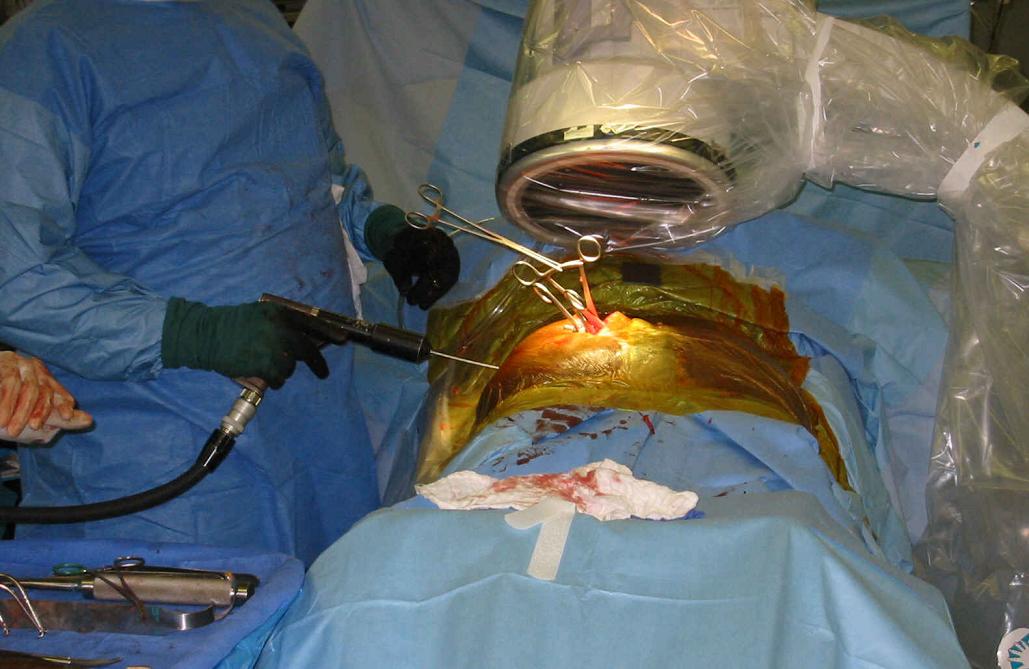
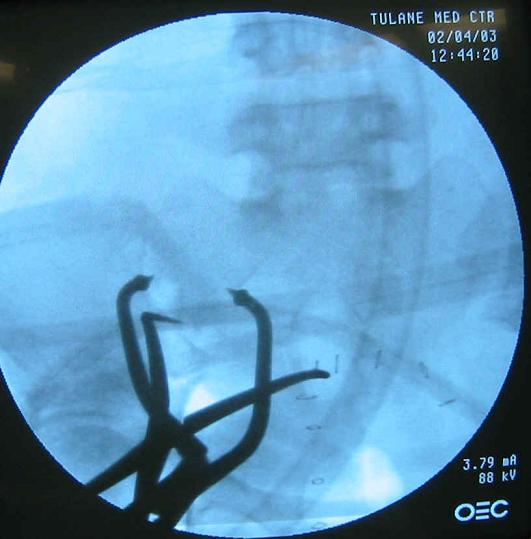
- consider a traction x-rays of extremity to help judge effects of ligamentotaxis on displaced articular fragments;
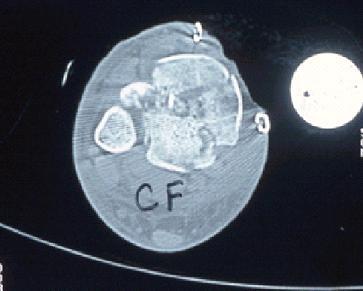
- CT scan: helps plan surgical fixation of articular fragments;
- note whether fibula is intact or fractured;
- w/ comminuted fibular fracture it is important to bring fibula out to length (talo-crural angle)
- w/ fibula intact, carefully evalute the syndesmosis;
- classification: and degree of articular comminution;
- type I: pilon frx
- type II: pilon frx
- type III: pilon frx
- type A:
- minimal or no anterior tibial cortical communition, two or more large tibial articular fragments,
and usually an oblique or transverse fibular fracture at level of the plafond (or ankle joint);
- type B:
- results from severe axial compression force, causing distal tibial bony impaction and comminution;
- Surgical Treatment:
- controversies:
- surgical timing and staged reconstruction;
- plate vs ex fix;
- ankle arthrodesis;
- primary arthrodesis is one consideration with severe injuries;
- references:
- Ankle arthrodesis using antegrade intramedullary nail for salvage of nonreconstructable tibial pilon fractures.
- Fracture reduction and primary ankle arthrodesis: a reliable approach for severely comminuted tibial pilon fracture.
- Primary Arthrodesis of the Tibiotalar Joint in Severely Comminuted High-Energy Pilon Fractures.
- initial treatment and timing of surgery
- current thinking: external fixation (with or without fibular fixation) followed by delayed definitive fixation at 12-24 days;
- Does a staged posterior approach have a negative effect on OTA- 43C fracture outcomes?
- Clinical and radiographic outcomes in patients operated for complex open tibial pilon fractures.
- Surgical Fracture Fixation: surgical technique:

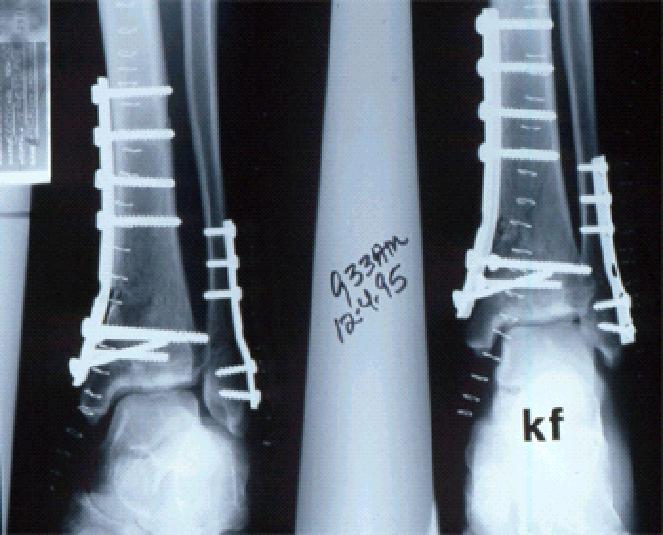
- reduction and ORIF of fibula;
- exposure of tibial articular surface
- restoration of tibial articular surface
- Treatment of AO/OTA 43-C3 Pilon Fracture: Be Aware of Posterior Column Malreduction.
- fixation of metaphysis to diaphysis:
- Risk Factors for Tibial Plafond Nonunion: Medial Column Fixation May Reduce Nonunion Rates.
- Implants:
- plate fixation
- IM Nail: (see Nail fixation of distal tibia)
- references:
- Is there a role for intramedullary nails in treatment of simple pilon fractures? Rationale and preliminary results.
- Intramedullary Nailing in a Tibial Shaft Fracture With Distal Articular Extension
- Distal metaphyseal fractures of the tibia with minimal involvement of the ankle. Classification and treatment by locked intramedullary nailing..
- [Combination of intramedullary nail and covered screw osteosynthesis for managing distal tibial fracture with ankle joint involvement].
- Extra-articular distal tibia fractures: a mechanical evaluation of 4 different treatment methods.
- Intramedullary nailing of unstable diaphyseal fractures of the tibia with distal intraarticular involvement.
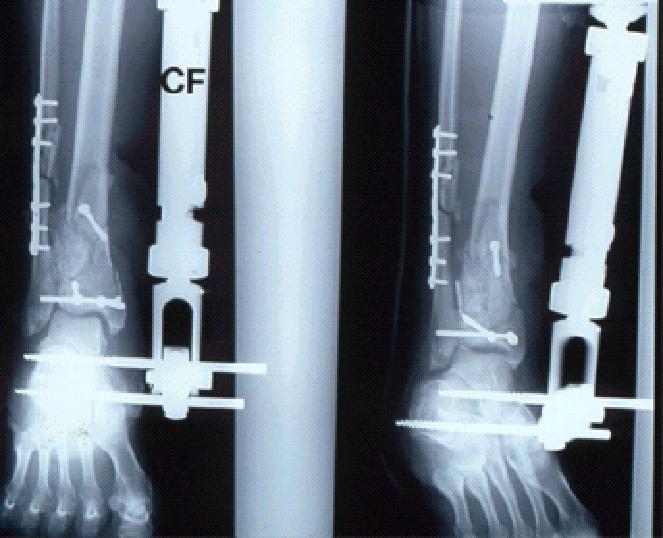
- uniplanar external fixation
- external fixation - foot inclusion
- circular wire fixators
- theoretically, there is some danger of osteomyelitis in having transfixation wires pass through the fracture segments
since incidence of pin tract infections in pilon fractures may be as high as 55%;
- other complications with circular wire fixators include ankle stiffness, swelling, RSD, and ankle tendon injury;
- references:
- Treatment of displaced pylon fractures with circular external fixators of Ilizarov.
- External Fixation Versus ORIF for Distal Intra-articular Tibia Fractures.
- cancellous bone grafting of metaphyseal defect
- wound closure:
- ref: The management of the soft tissues in pilon fractures.










- Complications:
- wound complications and infection: (see soft tissue coverage for tibia fracture)
- w/ tranditional early ORIF of the tibial articular surface the occurrance of wound slough and infection
has ranged from 10 to 50%;
- some feel that this complication can be minimized by delayed ORIF (once the swelling has diminish ed);
ed);
- 37% deep infection rate in tibial plafond Rüedi III (Teeny and Wiss (1993));
- unplanned surgery for complications (Wyrsch (1996))
- 55% for ORIF
- 18% for external fixation and limited ORIF
- degenerative joint disease:
- rates for secondary ankle arthrodesis after attempted ORIF of type 3 fractures approaches 30%.
- syndesmotic injuries:
- Syndesmosis and Syndesmotic Equivalent Injuries in Tibial Plafond Fractures.
- references:
- Open reduction and internal fixation of tibial plafond fractures. Variables contributing to poor results and complications.
- Complications encountered in the treatment of pilon fractures.
- Delayed wound healing, infection, and nonunion following open reduction and internal fixation of the tibial plafond fractures.
- The management of the soft tissues in pilon fractures.
- Early complications following the operative treatment of pilon fractures with and without diabetes.
- Operative Treatment of Fractures of the Tibial Plafond. A randomized, prospective study


 ***
*** 
![]()
Fractures of the tibial pilon.
Intraarticular "pilon" fracture of the tibia.
Pylon fractures of the distal tibia.
Pilon fractures of the tibia: a study based on 19 cases.
Fractures of the tibial plafond. Evolving treatment concepts for the pilon fracture.
Tibial pilon fractures: a comparative clinical study of management techniques and results.
Unilateral external fixation for severe pilon fractures.