

See:
- Discussion:
- indications:
- impingement syndrome
- patients w/ a stable impingement syndrome w/ good shoulder function should participate in a formal rehabilitation program for 6 months;
- patients w/ worsening pain and function may undergo early acromioplasty if the usual non op measures fail to relieve symptoms;
- cautions:
- concomitant cervical spondylosis or restricted shoulder motion may have worse results from acromioplasty than patients who are free of additional pathology;
- reference:
- Impingement syndrome in the absence of rotator cuff tear (stages 1 and 2).
- internal rotation contracture:
- limitation of external rotation worsens impingement syndrome since the greater tuberosity cannot clear the acromion as the arm is elevated;
- logically, by improving the internal rotation contracture, the impingement syndrome will be relieved;
- w/ concomitant massive rotator cuff tear, resection of CA ligament can lead to a loss of containment of humeral head causing anterior-superior migration;
- when the rotator cuff is not reparable, CA ligament as well as the anterior-inferior aspect of the acromion generally are to be preserved;
- Incision:

- incision is made in antero posterior direction between the tip of the acromion and the AC joint;
- this allows access to the AC joint and the cuff;
- if a distal clavicular incision is not planned then make the incision along the lateral border of the acromion;
- incision is carried down to the delto-trapezial fascia;
- subQ tissue overlying deltoid is completely mobilized (this allows exposure from distal clavicle to tip of acromion);
- two Gelpi rectractors in each end of the wound;
- Periosteal Incision:
- superficial dissection procedes down to the deltotrapezial fascia, at which time full thickness flaps are mobilized, leaving the fascia on the deltoid for later closure;
- deltoid "on" strategy:
- deltoid is split down the anterolateral raphe, and subsequently sharpey's fibers are elevated "en mass" from either side of the anterior acromion, which allows the acromioplasty to procede without having to take down the deltoid off of the acromion;
- deltoid "off" strategy:
- motivation for this technique: the "Rockwood" anterior acromioplasty ends up leaving a sizable defect which needs to be re-secured with full thickness deltoid sutures;
- if deltoid "on" technique (deltoid sparing) technique is used, then only dorsal deltoid fascia remains intact (which is weaker than a secure full thickness repair);
- full thickness fascia periosteal flap extending in a medial to lateral direction, starting at lateral edge of AC joint and extending directly laterally;
- it is important not to make this incision too far anteriorly since it will make it difficult to re-attach the deltoid at the end of the case;
- acromial branch of the thoracoacromial artery is coagulated;
- often it will be necessary to "dogleg" the peristeal flap incision posteriorly for additional exposure;
- a 15 blade scapel is then used to sharpley elevate the deltoid from its attachments on the anterior, lateral, and inferior aspects of the acromion;
- at the end of the case, it is essential that a secure deltoid repair be made;
- full thickness substance of deltoid is opposed to raw surface of acromion, by passing No 2 ethibond sutures through 2 or 3 drill holes made in acromial surface;
- Deltoid Incision:
- continue to incise thru the anterior fascial raphe of deltoid w/ cautery in line w/ the periosteal incision;
- stitch is made in deltoid, 4 cm below the lateral tip of acromion;
- using tonsil clamp bluntly dissect thru deltoid where it meets periosteal incision line.
- initially place tonsil, just under acromial edge & "pop" thru deltoid without injury the underlying rotatory cuff.
- spread through this interval and then spread apart deltoid fibers.
- insert a finger through this opening and then move it underneath the deltoid toward the marking stitch;
- use cautery over the underlying finger to complete deltoid exposure and dissection from the anterior acromion;
- finger is placed under the coracoacromial ligament is excised & undersurface of the acromion is exposed;
- deltoid paddles are placed into substance of deltoid;
- Acromioplasty:
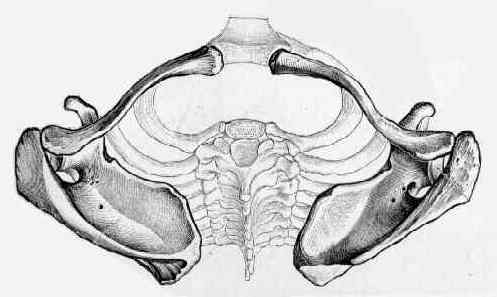
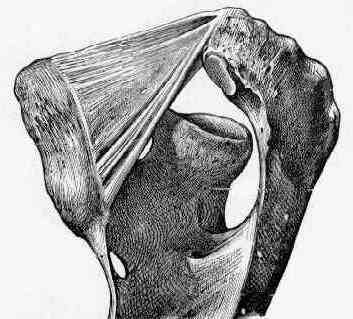
- coraco-acromial ligament:
- some advocate division of the ligament, feeling that it is an integral part of the impingement syndrome;
- some feel that excision of the CA ligament leads to postop weakness;
- w/ a potential irrepairable cuff tear, consider leaving the CA ligament intact;
- intact ligament helps prevent superior migration of humeral head;
- spade may be placed underneath acromion for protection (but this may not be possible when the CA ligament is not transected);
- references:
- The coracoacromial ligament: morphology and study of acromial enthesopathy. 
- Contact pressure and glenohumeral translation following subacromial decompression: how much is enough?
- Codman acromioplasty:
- mentioned for historical purposes;
- involves lateral acromioplasty or total acromionectomy;
- Neer acromioplasty:
- emphasis is placed on resection of the inferior prominence of the acromion;
- this technique has been criticized since it may allow residual impingement of the anterior acromion;
- Rockwood acromioplasty:
- involves a two step acromioplasty;
- first, portion of anterior acromion which protrudes beyond the anterior edge of the clavicle is resected;
- usually this translates to resection of about 5 mm of the anterior acromion;
- second, undersurface of the acrmion may be smoothed or beveled to convert it to a type I acromion;
- generally, the remaining anterior acromion should be thinned down to 8 mm in thickness;
- this is consistent with Synder system for acromial thickness (type A (less than 8 mm), type B (8.1 to 12 mm), and type C (greater than 12 mm));
- nasal rasp is used to further smooth undersurface;
- Distal Clavicular Resection:
- only performed when specifically indicated, since patients can expect a significantly longer rehab time;
- according to Rockwood and Lyons, distal clavicular excision was required in only 6% of patients;
- complete periosteal dissection across AC joint;
- strip peristeal flaps both anteriorly and posteriorly;
- small homan retractors on either side of distal clavicle;
- palpate the conoid and trapezoid ligaments;
- transect 1 to 1.5 cm of distal clavicle;
- elevate one corner of the distal clavicle and subperiosteally dissect from the clavicular fascia;
- The influence of distal clavicle resection and rotator cuff repair on the effectiveness of anterior acromioplasty.
- Shoulder impingement syndrome: diagnosis, radiographic evaluation, and treatment with a modified Neer acromioplasty.
- Bursectomy: (see arthroscopic subacromial bursectomy)
- bursa is now exposed;
- using facial scissors, remove the bursa from posterior to anterior, having the assistant rotate the arm to assist w/ bursectomy;
- Biceps Release and/or Tenodesis:
- often indicated for concomitant rotator cuff tear, subluxation, and for degenerative changes in the intra-articular portion of the tendon;
- biceps tenodesis is most indicated when more than 50% of the tendon is eroded;
- tendon hypertrophy is not be itself an indcation for tenodesis;
- Greater Tuberosity Debridement:
- prominent tuberosity can be excised if there is further impingment;
- Failed Acromioplasty / Rotator Cuff Surgery:
- Failed anterior acromioplasty. A review of 51 cases.
- On the disadvantages of radical acromionectomy.
- Failed acromioplasty for impingement syndrome.
Shoulder impingement syndrome: diagnosis, radiographic evaluation, and treatment with a modified Neer acromioplasty.
Acromioplasty for impingement with an intact rotator cuff.
Subacromial impingement decompressed with anterior acromioplasty.
Anterior acromioplasty for subacromial impingement in patients younger than 40 years of age.
Arthroscopic subacromial decompression versus open acromioplasty. A two-year follow-up study.
Conservative open anterior acromioplasty.
Arthroscopic acromioplasty. Technique and results.
Open Rotator Cuff Repair without Acromioplasty.
Arthroscopic Decompression with Acromioplasty and Structured Exercise Was No More Effective and Was More Expensive Than Exercise Alone