

- Case Example by Dr. James R. Urbaniak MD
- Equipement:

- 4 mm 30 deg endoscope;
- hook knife;
- slotted cannula;
- long cotton padded Q tips;
- Anesthesia:
- ensure that lidocaine does not contain epinephrine;
- median nerve block may be useful but does not allow the patient to demonstrate activity of the motor branch at the end of the case;
- local injection over proximal and distal incisions, but avoid infiltrating lidocaine in mid palmar area;


- Positioning:
- supine w/ arm on hand table;
- mark out landmarks;
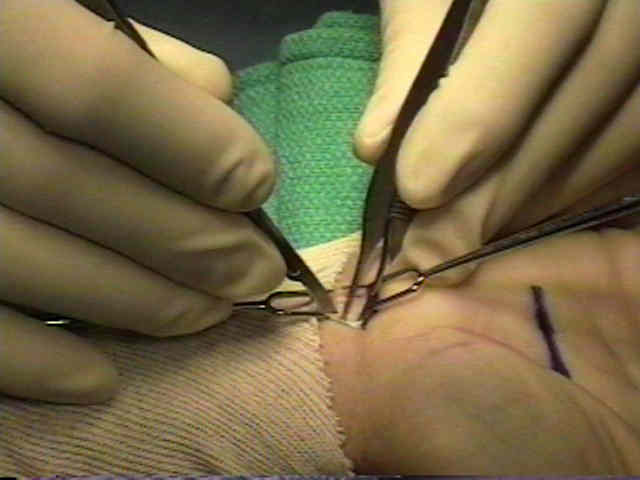
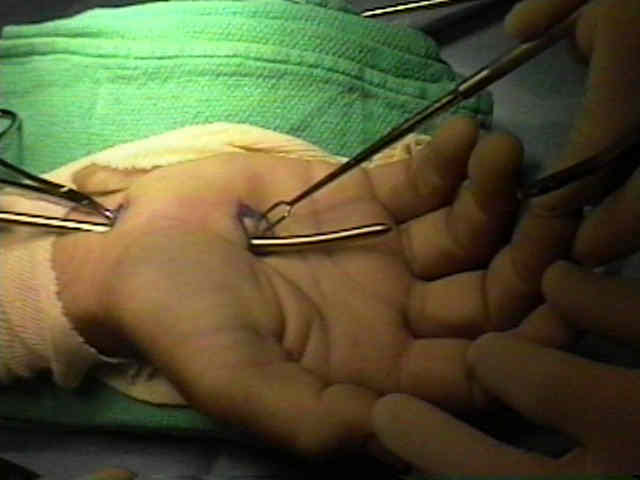
- Proximal Incision:
- just proximal to the proximal wrist flexion crease along the ulnar border of the palmaris longus;
- a proximally based flap of superficial fascia is created and is elevated w/ a small clamp;
- immediately underneath this fascia lies the median nerve;
- probing the undersurface of the TCL should give a washer-board sensation;
- if washer-board sensation is not present then the probe is either in Guyon's Canal or is superficial to the TLC;


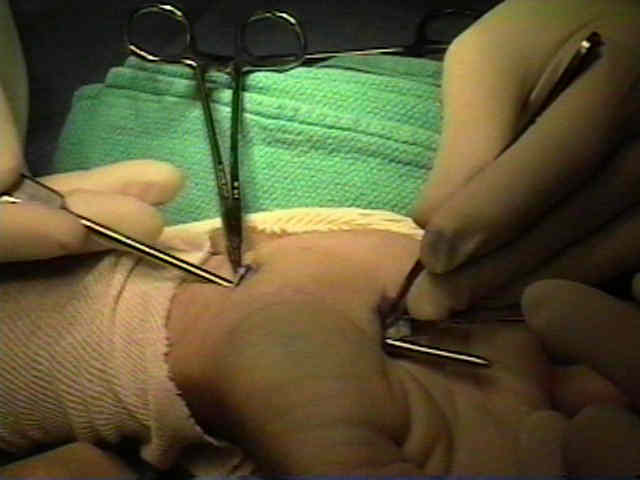
- Distal Incision:
- just distal to the distal edge of the transverse carpal ligament
- a blunt tipped obturator is placed into the carpal tunnel and is pushed distally to the distal border of the TCL;
- hazards include the superficial palmar arch;
- wrist flexion draws the superficial palmar arch away from the TCL;
- the tip of the obturator is then gently pushed upwards so that its tip can be palpated underneath the skin (just distal to the TLC);
- this tip marks the proper location for the distal incision;
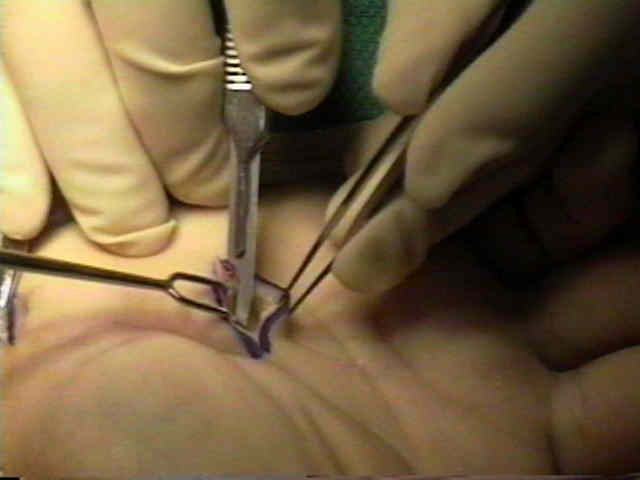

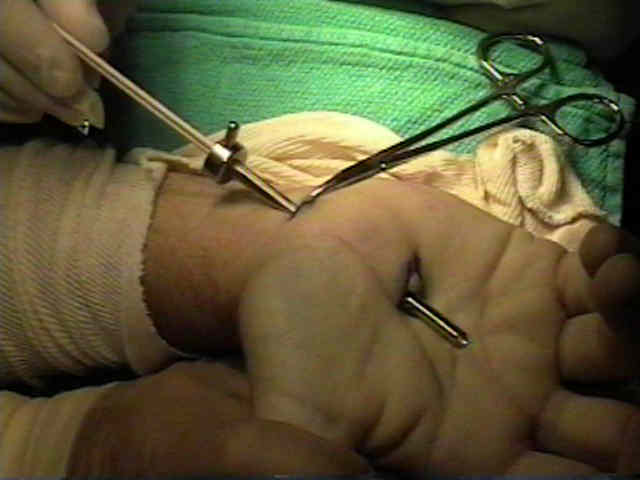
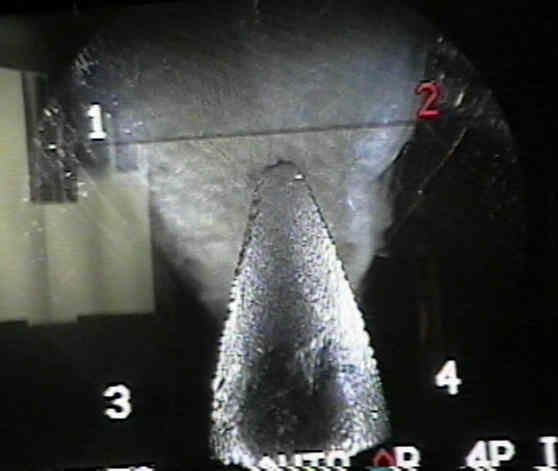
- Preparation for TCL Transection:
- blunt antatomy probe is used to gently probe the undersurface of the TLC;
- the "washer board" feel of the undersurface of the TLC helps confirm that the probe lies within the carpal tunnel;
- carefully pass sequentially larger dilators into the carpal tunnel;
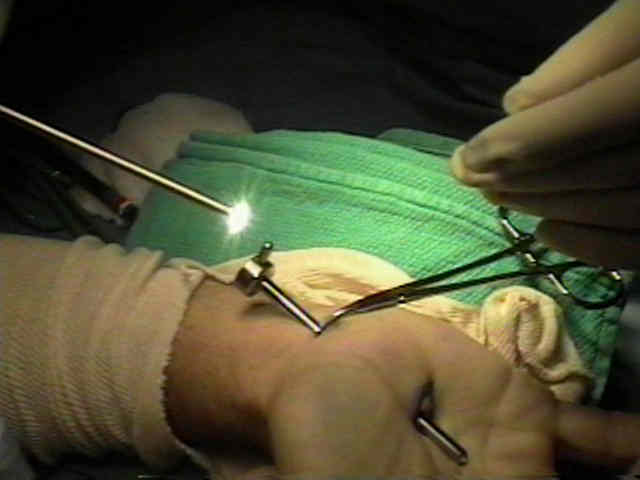
- slotted cannula is placed into distal incision and into the carpal tunnel, w/ the slot point slightly to Guyon's Canal (about 11 o'clock), and parallel to the patient's arm;
- extension of the patients thumb, places tension on the TLC, facilitating transection;
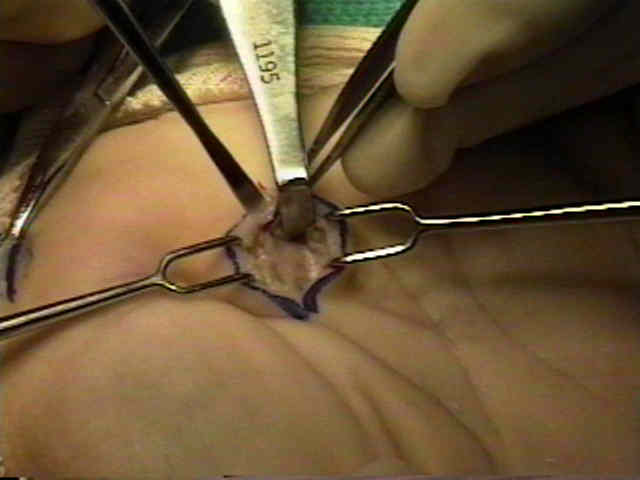
- just distal to the TCL, a superficial layer of subcutaneous fat is seen;
- sterile Q tips are used to clean the undersurface of the TLC;
- reference:
- A simple technique for identification of the distal extent of the transverse carpal ligament during single-portal endoscopic carpal tunnel release.



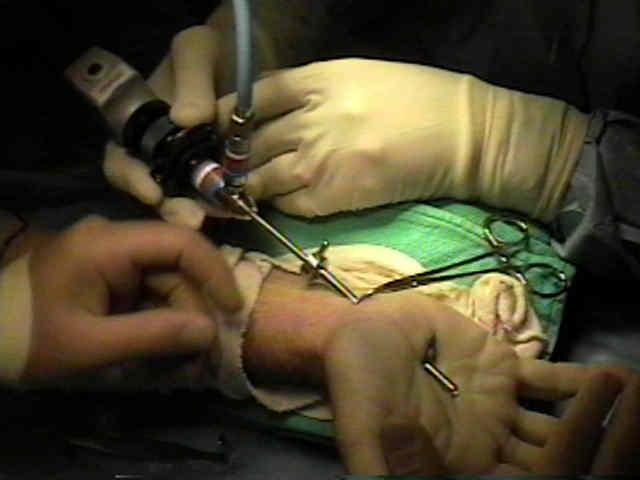
- Transection of TLC:
- the hook knife is placed into the obturator which already lies with in the distal incision;
- the blade is inserted into the mid-aspect of the TLC;
- the blade is then pulled from proximal to distal
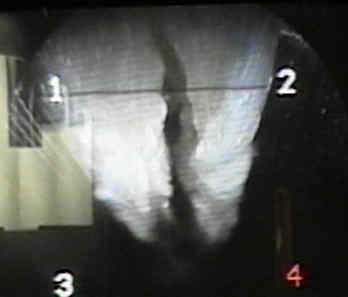
- the cannula and arthroscope positions are reversed;
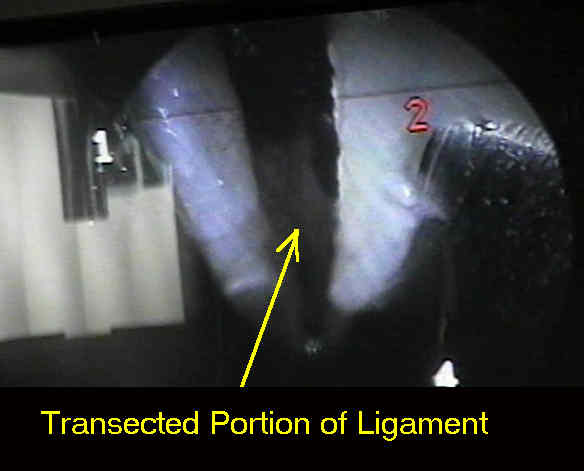
- the blade is placed in the mid aspect of the TLC (where the TLC was first transected) and then under direct vision, the blade is pulled from proximal to distal;







- Transection of the Palmar Fascia:
- incomplete release of the palmar fascia is a common cause for recurrent CTS;
- take care to avoid injury to the palmar cutaneous branch (radial side) and the ulnar artery (ulnar side)


The ulnar neurovascular bundle at the wrist. A technical note on endoscopic carpal tunnel release
Carpal arch alteration and related clinical status after endoscopic carpal tunnel release.
Endoscopic carpal tunnel release.
Carpal Tunnel Release. A Prospective, Randomized Assessment of Open and Endoscopic Methods.
Endoscopic carpal tunnel release: an anatomic study.
Anatomic relationships of an endoscopic carpal tunnel device to surrounding structures.
Endoscopic carpal tunnel release: an anatomic study of the two-incision method in human cadavers.
Endoscopic release of the carpal tunnel: a randomized prospective multicenter study.