

 - Discussion, Indications and Outcomes:
- Discussion, Indications and Outcomes:- impingement syndrome
- open acromioplasty
- what exactly does an acromioplasty do?
- [Subacromial denervation as a treatment modality for patients with subacromial pathology]
- Initial Set Up:
- prior to inserting instruments into subacromial space it is helpful to prevent subacromial bleeding
(or limit it before it occurs);
- pre-inject the subacromial space with an epinephrine containing solution;
- consider adding 1/2 ampule of epipnephrine to each 3 liter bag of NS;
- ensure that multiple fluid bags are ready;
- ensure that intra-articular cautery is ready;
- Subacromial Bursal Debridement:
- Arthroscopic Decompressions:
- posterior portal is used to view the subacromial space, the lateral portal is used for instrumentation, and anterior portal is used
for either outflow or inflow;
- a 6.5 mm cannula is inserted thru the anterior and lateral portals to accomadate the inflow and instrumentation;
- first step usually involves a limited bursectomy using the 5.5 mm full radius shaver;
- it is essential to limit the bursectomy to the region around the anterior acromion, inorder to limit bleeding;
- establish landmarks:
- the anterior portal serves as a landmark for the AC joint;
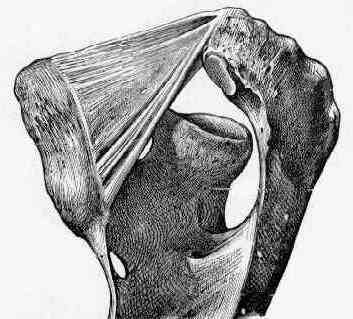
- undersurface of acromion is covered by periosteal layer & layer of coracoacromial ligament, which extends under acromion
(this thick and extensive);
- entire undersurface of the antero-lateral acromion is cleared of soft tissue using intra-articular cautery inorder to limit bleeding;
- take care not to stray into the deltoid fibers, since this will stir up bleeding and will ruin the case;
- once bursal tissue is removed from undersurface of acromion, then remove bursal tissue and deltoid attachements
on anterior acromial surface;
- note that bleeding from branch of thoracoacromial artery can easily occur when sectioning the coracoacromial ligament;
- Acromioplasty:
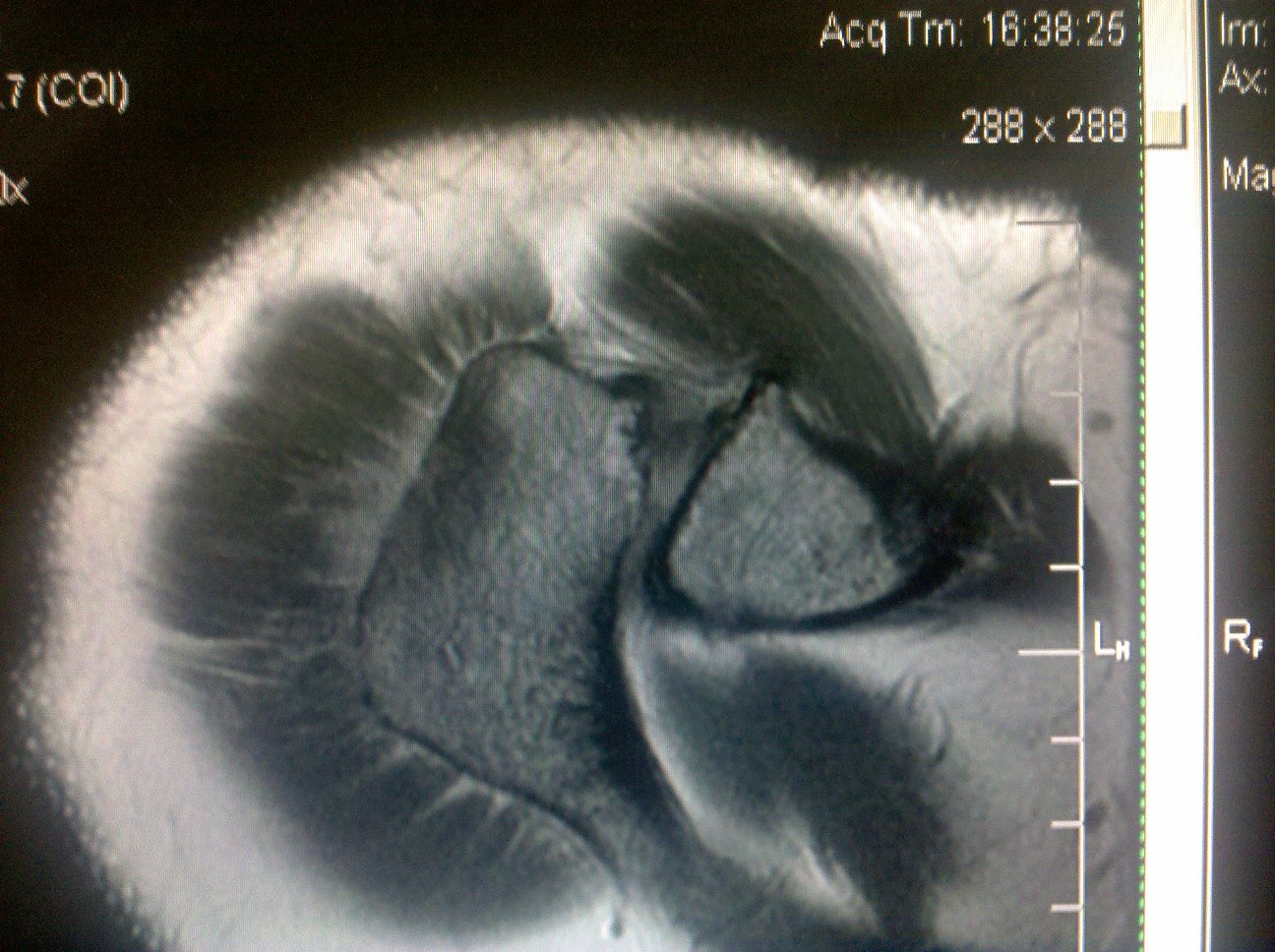
- arthroscopic impingement test:
- following removal of the inflamed bursal tissue an arthroscopic impingement test should bes performed;
- place the arthroscope through the lateral arthroscopic portal and then flex the shoulder (move back and forth from the
scapular plane to straight forward);
- note any impingement between the humeral head and the acromion (following the acromioplasty no impingement should be
observed and the subacromial space should be maintained);
- controversies:
- full thickness acromioplasty: risks detachment of the deltoid insertion or fully resecting coracoacromial ligament
- goals:
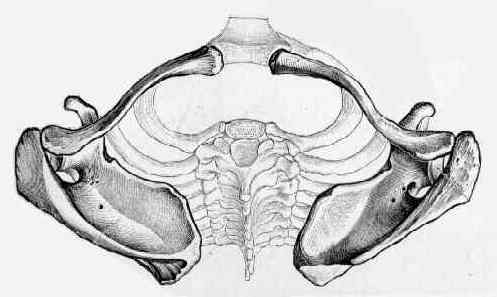
- convert a pathological coracoacromial arch to a physiological arch;
- usually it may be necessary to remove only 5 mm to 8 mm (use anterior deltoid periosteal fibers (white) as a guide) with a
goal to maintain an interval between the acromial and humeral head to about 15 mm;
- maintain the superior deltoid fascial attachments
- release but not resect the CA ligament
- “Limited Anterior Resection” Technique
- goal is not to produce a completely flat undersurface but to perform a smooth and even taper
- references:
- The relationship between clinical outcomes and the amount of arthroscopic acromial resection.
- Intraoperative measurements of the subacromial distance.
- Arthroscopic rotator cuff debridement without decompression for the treatment of tendinosis.
- No difference in long-term development of rotator cuff rupture and muscle volumes in impingement patients with or without decompression
- Controversies: Is Acromioplasty required with Arthroscopic RTC Repair?
- Controversies: rotator cuff repair and distal clavicle excision: (see distal clavicle excision)
- in the study by Fischer BW, et al (1999), the authors studied the effect of violation of the AC joint during arthroscopic
acromioplasty;
- found that patients that either had no violation of the AC joint or patients that had complete DCR had no postop sequelae
in reference to AC joint;
- in contrast, 14 / 36 shoulders (39%) w/ documented AC joint violation and a partial DCR developed AC joint symptoms at
an average of 8.4 months;
- authors recommend an all or nothing approach to the AC joint (ie avoid partial distal clavicle resection);
- recommended that if AC joint must be violated to perform an adequate decompression of the subacromial space,
complete resection of the distal clavicle should be performed, even if the radiographs show no preoperative
degenerative changes;
- authors theorize that partial distal clavicle excision increases AC joint motion in all planes, especially rotation and superior
translation, after co-planing of the inferior surface;
- these authors proposed that the increased mobility could lead to acromioclavicular joint symptoms in a previously
asymptomatic joint or accelerate symptoms in a joint with mild symptoms before surgery;
- references:
- Incidence of Acromioclavicular Joint Complications After Arthroscopic Subacromial Decompression.
- Acromioclavicular joint reoperation after arthroscopic subacromial decompression with and without concomitant acromioclavicular surgery.
- Controversies: Is Acromioplasty required with Arthroscopic RTC Repair?
- posterior capsular release:
- may be indicated in selected patients, w/ limited internal rotation and w/ thickened posterior capsule who demonstrate
persistent impingement (as seen arthroscopically);
- technique involves arthroscopic visualization from the anterior portal and release of the posterior capsule off of the glenoid
using cautery;
- references:
- Recognition and Treatment of Refractory Posterior Capsular Contracture of the Shoulder
- Arthroscopic acromioplasty for lesions of the rotator cuff.
References:
Arthroscopic subacromial decompression versus open acromioplasty. A two-year follow-up study.
Arthroscopic acromioplasty. Technique and results.
Arthroscopic debridement versus open repair for rotator cuff tears. A prospective cohort study.
Partial thickness rotator cuff tears: results of arthroscopic treatment.
Arthroscopic treatment of massive rotator cuff tears. Clinical results and biomechanical rationale.
Rotator cuff pathology. Arthroscopic assessment and treatment.
Arthroscopic subacromial decompression: results in advanced impingement syndrome.
Shoulder impingement syndrome in athletes treated by an anterior acromioplasty.
Does arthroscopic acromioplasty provide any additional value in the treatment of shoulder impingement syndrome?: a two-year randomised controlled trial.
Reversed arthroscopic subacromial decompression for symptomatic irreparable rotator cuff tears: Mid-term follow-up results in 34 shoulders
[Subacromial denervation as a treatment modality for patients with subacromial pathology]