

- See:
- Anterior Approach to the Humerus
- Axillary Approach:
- Posterior Approach
- Posterior Approach to Humerus
- Surgical Approach for Proximal Humeral Fractures
Positioning and Draping:
- supine or beach chair;
- small soft bolster is placed beneath the shoulder blades to protract the shoulder;
- head is stabilized to prevent hyperextension and subsequent brachial plexus palsy;
- place patient in a beach chair position w/ torso flexed 45 deg and the knees flexed to 30 deg;
- in the beach chair position, ensure that the patient is firmly fastened to prevent sliding;
- move patient to the edge of the table (operative side), and use a McConnel positioner to prevent the patient from failing off the table;
- positioning is optimal when the scapula hangs over the edge of the table;
- place a folded towel under the spine and ipsilateral scapula;
- it is helpful to drape the should w/ a large Ioband sheet w/ a hole cut in the middle;
- several Iobrand strips (2-3 inches in width) are also helpful;


- consider the Mconnel Shoulder Positioner;



- consider the Mconnel Shoulder Positioner;
- several Iobrand strips (2-3 inches in width) are also helpful;



Instruments:

- Balfour Self Retaining Retractor;
- Homan Retractors:
- Fukuda Humeral Head Retractor:
- Gelpi retractors;
{kind=link}
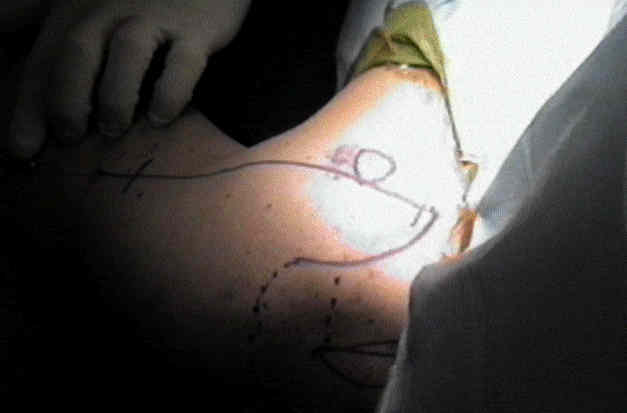
Superficial Dissection:

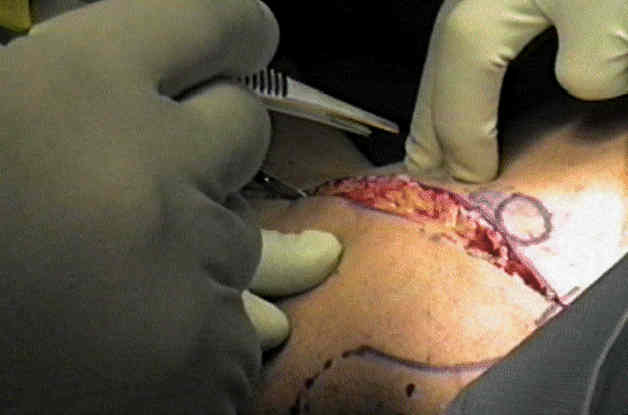

Deep Dissection:
- clavipectoral fascial incision:
- once the deltopectoral interval has been fully developed, the clavipectoral fascia is exposed (which is most prominent lateral to coracoid muscles);
- clavipectoral fascia is differentiated from the deeper tissues, because it will not move with internal and external rotation;
- tip of the coracoid and the conjoined tendon (short head of biceps and the coraco-brachialis) is identified;
- clavipectoral fascia is then divided vertically just lateral to the conjoined tendon, up to coracoacromial ligament, exposing subscapularis tendon & lesser tuberosity.
- proximally, the fascia is divided at a point just lateral to the coracoid;
- the incision is carried distally to the level of the anterior circumflex;
- these vessels mark the level of the subscapularis tendon;
- identification of the musculocutaneous nerve:
- musculocutaneous nerve can usually be palpated on deep surface of coracobrachialis;
- nerve enters posterior of coracobrachialis about 5 cm distal to coracoid tip but can be as close as 1 to 2 cm;
- identification of the axillary nerve
- retraction:
- often a "Charnley type" of self retaining retractor is inserted underneath the deltoid medially and the coracobrachialis laterally;
- coraco-acromial ligament:
- in patients w/ traumatic arthritis or DJD, the shoulders may be tight and therefore, the ligament can be
partially incised for better exposure of the upper portion of the subscapularis; - in patients w/ rheumatoid arthritis or cuff tear arthropathy, excision of the CA ligament may destabilize the shoulder arthroplasty;
- in patients w/ traumatic arthritis or DJD, the shoulders may be tight and therefore, the ligament can be
Transection of the Subscapularis:
- subscapularis tendon and the underlying joint capsule are divided approximately 1 cm medial to the lesser tuberosity;
- medial retraction of the tendon and capsule will expose the glenoid;
Caspsular Transection:
- external rotation of the humerus affords better capsular exposure and relaxes the nerve;
- insert a blunt retractor inferiorly to protect the axillary nerve, insert two single pronged skin hooks to elevate the capsule superiorly and place it under tension;
- vertically transect the capsule at a point midway between the lesser trochanter and the edgle of the glenoid;
- carry this vertical capsular incision superiorly into the rotator interval, which converts the capsular incision into a T (since the rotator interval lies in a horizontal direction);
- at the end of the case, the superior and inferior capsular capsular flaps are closed (and shortened) in order to shift the inferior capsule in a superior direction;
- the vertical portion of the incision is closed anatomically (so that there will be no loss of external rotation);
Distal Exposure:
- lower part of shaft is exposed by incising brachialis longitudinally along lateral border of biceps;
- lowest part of the front of the shaft can be approached between brachioradialis which is retracted laterally and brachialis which is retracted medially