


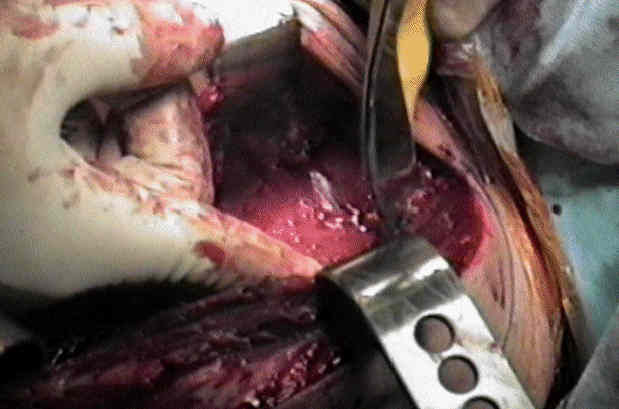
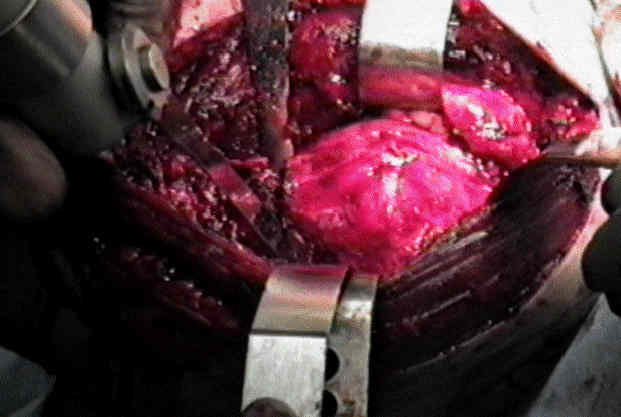
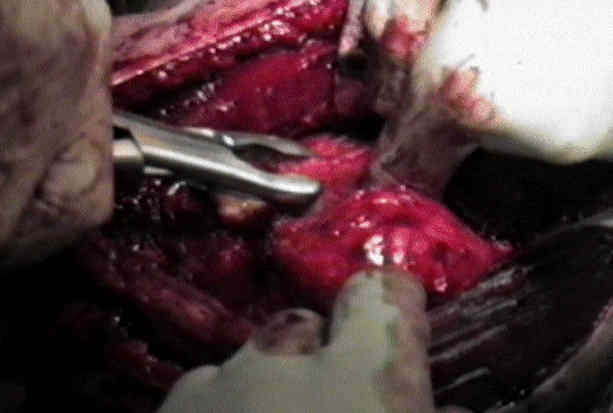
- Exposure of the Subscapularis:
- the upper portion of the subscapularis tendon is exposed by partial release of the CA ligament off the coracoid, by placement of a Homan retractor directly above the coracoid, and by abduction and external rotation of the arm;
- the upper portion of the subscapularis tendon lies immediately below the tip of the coracoid process;
- the lateral insertion of the subscapularis is identified just medial to the bicipital groove;
- the inferior portion of the subscapularis can be hidden by the pectoralis tendon insertion;
- if this is the case, incise the superior 1 cm of the insertion;
- the inferior portion has two portions: a tendinous and a muscular portion;
- the AHCA helps demarcate these portions;

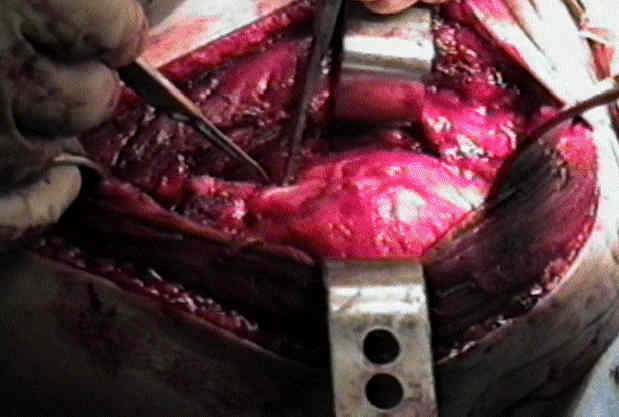
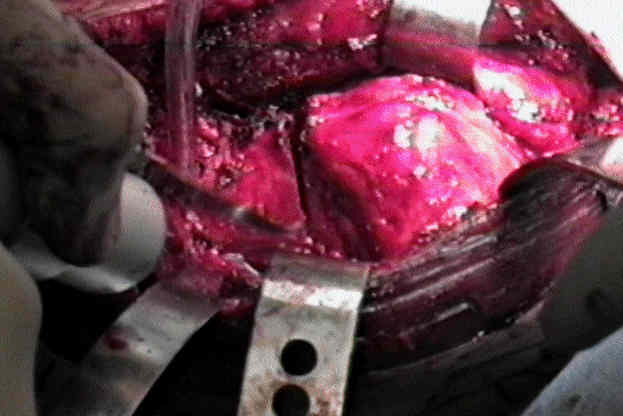
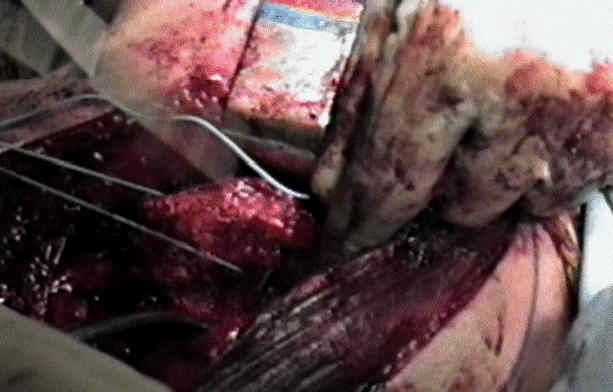
- Subscapularis and Anterior Capsule Incision:
- externally rotate the shoulder, w/ the arm adducted;
- place 2-3 stay sutures in the tendon 2 cm from the bicipital groove;
- prior to incising the subscapularis, attempt to palpate for the axillary nerve by passing the finger along the anterior surface of the inferior subscapularis;
- incise through the subscapularis tendon 1.5 cm medial to its origin;
- include the shoulder capsule in the dissection;
- superiorly, preserve the coracohumeral ligament;
- inferiorly, preserve the muscular portion of the subscapularis which lies below the AHCA;
- cautions:
- repair of the subscapularis to its tendinous stumpt may work well in patients w/ weak tissues (such as rheumatoids);
- alternatively, use cautery to incise the subscapularis directly off the bone, and repair the scapularis through drill holes at the end of the case;
- in 4 part fractures, it may be necessary to remove the subscaplaris along with a small portion of bone;
- in this case curved scissors are used to incise the bicipital sheath, and expose the biceps tendon upto the supraglenoid tubercle, to better define the lesser and greater tuberosities (and their respective cuff insertions);
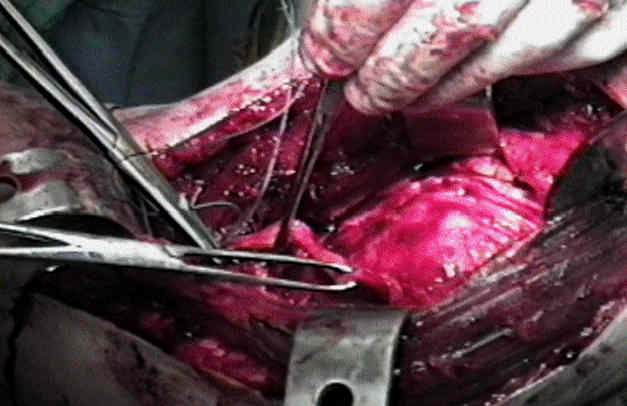
- division of humeral head:


- the greater and lesser tuberosity fragments are mobilized and freed of attached scar tissue to allow for tension free repair;
- (anchoring the greater and lesser tuberosities at the end of the case):
- ref: Lesser tuberosity osteotomy for total shoulder arthroplasty. Surgical technique.
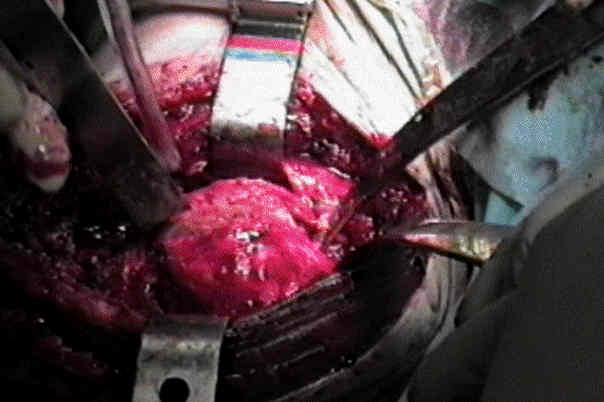
- Mobilize the Subscapularis
- subscapularis and anterior capsule off the anterior glenoid, and then temporarily stuff the tendon between the glenoid and the muscle belly;
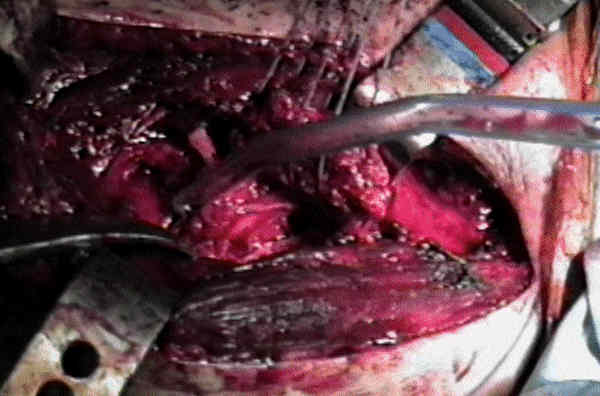
- Transect the Remaining Subscapularis:
- a Fukuda retractor is then placed anterior to humeral head and just behind the posterior glenoid, in order to sublux the humeral head posteriorly and laterally;
- this places the remaining subscapularis (muscular portion) under tension, which facilitates dissecting this remaining muscle off the bone;
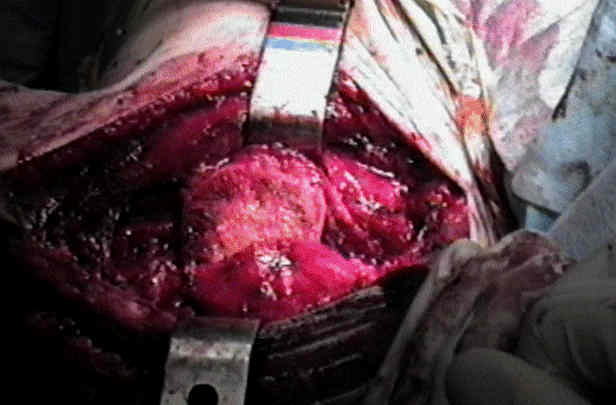
- placing the arm in abduction and external rotation will also increase tension on the remnant portion of the subscapularis;
- as the remaining subscapularis and capsule are dissected off the humerus, taken care to avoid injury to the axillary nerve as it passes to the quadrilateral space
A surgical tip for shoulder hemiarthroplasty in a patient with a deficient rotator cuff.