

- Evaluation of Muscle:
- about 5% of shoulders that have had an anterior dislocation will sustain a irrepairable injury to the subscapularis, which will contribute to
further instability;
- in this case, a pectoralis transfer would be indicated;
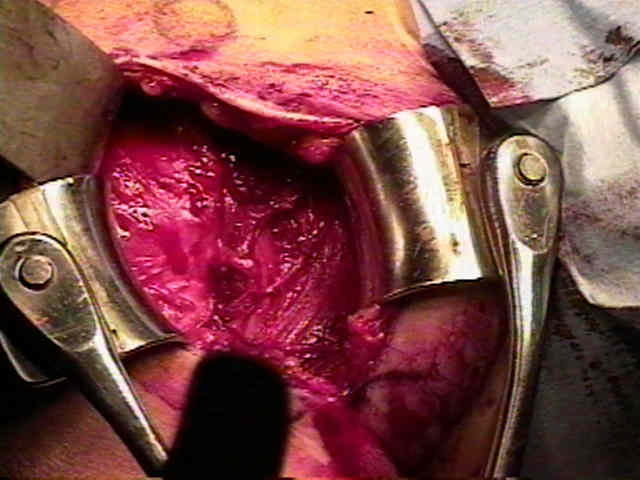
- Preparation:
- identify the anterior humeral circumflex vessels (three sisters) at the inferior aspect of tendinous portion subscapularis;
- note that the axillary nerve passes just inferior to the three sisters
- the nerve goes on to courses toward quadrangular space;
- a spade retractor can be placed just above the three sisters to protect the axillary nerve;
- alternatively a Joker can be inserted deep to the joint capsule at a point just lateral to the superior border of the subscapularis;
- the Joker will then pass out of the joint capsule at the inferior border of the subscaularis tendon - just above the 3 sisters;
- again the point of this is to protect the axillary nerve;
- before an incision is made in the subscapularis, the arm should be externally rotated to avoid damage to axillary nerve and circumflex
vessels;
- prior to incision into the subscapularis tendon, appropriate retractors need to be in place, which allows indentification of the insertion of the
subscapularis, and its superior and inferior borders;
- note: in a minority of patients with anterior instability, the subscapularis will be avulsed from the lesser tuberosity or may have a tear in the
the distal half of subscapularis tendon;


- Subscapularis Transection:

- the subscapularis insertion is comprised of a tendinous portion occupying the proximal 2/3 and a muscular portion occupying the
inferior 1/3;
- generally only the tendinous portion requires transection, whereas the muscular portion is preserved inorder to protect the AHCA and
underlying axillary nerve;
- the vertical incision thru the tendinous portion of the subscapulais tendon is usually made 1-2 cm medial to its insertion on the lesser
tuberosity to facilitate subscapularis closure at the end of the case;
- a more medially placed verticle incision will make it easier to separate the subscapularis from the underlying capsule;
- it is usually necessary to retract the coracohumeral ligament superiorly inorder to complete the transection of the subscapularis
tendon;
- the lateral portion of the subscapularis tendon is elevated off the underlying capsule to facilitate closure at the end of the case;
- Subscapularis Elevation:
- medially, the subscapularis tendon is reflected off the capsule using cautery;
- insert two or three tagging sutures just medial to the line of transection, which will facilitate retraction;
- the underlying joint capsule can be perserved by leaving some fibers of the subscap attached to the capsule, as the subscapularis is
dissected medially;
- the tendon is elevated off the joint capsule w/ use of a periosteal elevator or scissors, and with constant tension on the sutures;
- as the dissection procedes medially the subscapularis will be less adherent to the underlying capsule and should be gently separated
past the glenoid;
- the remaining intact muscular portion of the subscapularis should be gently separately from the underlying capsule with care not to injure
the axillary nerve;
- once the subscapularis is transected, it can be retracted medially, but take care not to place excessively traction on the axillary nerve