


- Discussion:
- patient may note new onset of anterior knee pain;
- diagnosis may be difficult if frx is non-displaced;
- if patient is more than 6-12 months post-op, then consider bone scan;
- Etilogy:
- devascularization of the patella (as might occur from a lateral retinacular release which sacrifices the superior-lateral geniculate artery);
- use of single central fixation peg causing incr patellar strain;
- use of bone cement due to heat necrosis
- high patellar strains due to component malignment;
- increased thickness of the patellofemoral articulation (from excessively thick patella, oversized femoral component, or anterior translated femoral component);
- Management:
- determined by function of extensor mechanism & patellar implant fixation;
- most TKR patellar frx are vertically aligned and most do not have disruption of the extensor mechanism;
- patients with a significant extensor lag or a displaced frx will need surgery;
- Nonsurgical Treatment:
- indicated if extensor mechanism is intact, patellar component is secure, there is no comminution, & displacement is < 2 cm;
- undisplaced or minimally displaced frx not involving patellar component & presenting w/ a minimal extensor lag are rx'ed w/ 6 wks of
immobilization followed by progressive ROM;
- Surgical Treatment:
- w/ a comminuted frx, consider patellectomy or partial patellectomy;
- comminuted frx w/ a loose component are rx w/ patellectomy and extensor mechanism repair;
- partial patellectomy is indicated if there is single large fragment and a secure component;
- technique:
- patella frx w/ displacement of patellar button, requires excision of loose component & associated cement;
- displaced patellar frx w/ extensor lag & no involvement of patellar component are treated w/ ORIF of patella & repair of retinaculum;
- often only fixation that can be used is cerclage wire;
- immobilization for six weeks is recommended
- inadequate bone stock may prevent prosthetic replacement;
- outcomes:
- in the report by Ortiguera CJ, et al, the authors conducted a retrospective review of 85 patella fractures
(in 77 patients) following 12,464 consecutive total knee arthroplasties performed between 1985 and 1998;
- 78 fractures occurred after primary TKA and seven, after revision TKA;
- fractures were classified according to three main criteria:
- integrity of the extensor mechanism, fixation status of the patellar implant, and quality of the remaining bone stock;
- 38 fractured patellae had a stable implant and an intact extensor mechanism (Type I);
- all but one were treated nonoperatively, and there was only one late failure of nonoperative treatment, which required operative intervention;
- 12 fractures were associated with disruption of the extensor mechanism (Type II);
- 11 were treated operatively; six knees had complications and five had a reoperation.
- 28 fractures occurred in association with a loose patellar component (Type III);
- 20 were treated operatively; nine knees had complications, and four had a reoperation
The effect of alignment of the implant on fractures of the patella after condylar total knee arthroplasty.
Fracture of the patella after total knee arthroplasty.
The treatment of patellar fractures after total knee arthroplasty.
Patellar fracture type and prognosis in condylar total knee arthroplasty.
Patellar component failure in cementless total knee arthroplasty.
The treatment of patellar fractures after total knee arthroplasty.
Patellar fractures in total knee arthroplasty.
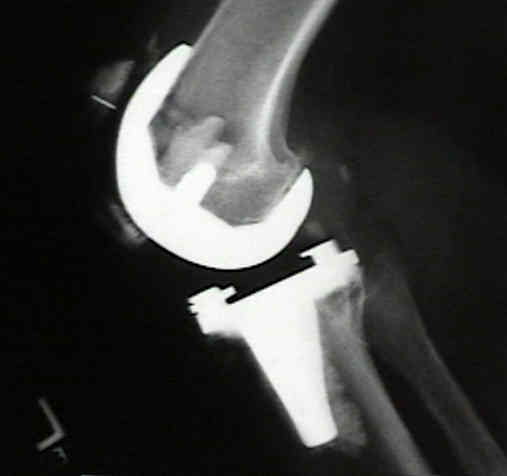
Patellar Fracture After Total Knee Arthroplasty