

- See:
- Anatomy
- Biomechanics
- Classification of Patellar Fractures
- Osteochondral Frx
- Pediatric Patellar Avulsion Fractures
- Discussion:
- classification of patellar fractures
- mechanism:
- direct trauma frequently produces stellate frx pattern and may be assoc w/ compromised anterior skin and subcutaneous tissue;
- associated injuries:
- PCL tear:
- ref: Concomitant posterior cruciate ligament injuries with direct injury-related patellar fractures
- Radiographs:
- AP view:
- patella may be difficult to see on AP view;
- peripheral fractures (osteochondral frx) may be confused w/ bipartite patella;
- radiographs of contralateral knee can help in this differentiation because bipartite patella rarely occurs unilaterally;
- lateral view:
- best reveals the comminution of frx or separation of fragments;
- w/ separation of the fracture more than 3-4 mm may is usually associated w/ retinacular disruption and loss of active extension;
- w/ patellar comminution at the inferior pole, consider partial patellectomy;
- some vertical frxs are best seen on tangential or Merchant radiographs;
- CT or other advanced imaging techniques are usually unnecessary;
- bone scans have been used to help to identify stress fractures;
- Non Operative Rx:
- indications:
- for undisplaced frxs w/ intact articular surface;
- preserved extensor mechanism w/ maintained active extension against gravity;
- retinacula on either side of patella should not be torn, as evidenced by pt's ability to maintain knee extended against gravity;
- there should be minimal displacement of fragments (2-3 mm)
- minimal disruption of the articular surface (2-3 mm)
- transverse undisplaced fracture of the patella is an avulsion frx;
- should aspirate with occurrence of tense hemotoma;
- Operative Treatment Options:
- indications:
- extensor mechanism is avulsed from the patella;
- displaced transverse fracture, either simple or comminuted, w/ associatted disruption of quadriceps retinacula;
- patellar frxs w/ compromised overlying skin should undergo delayed fixation;
- treatment options:
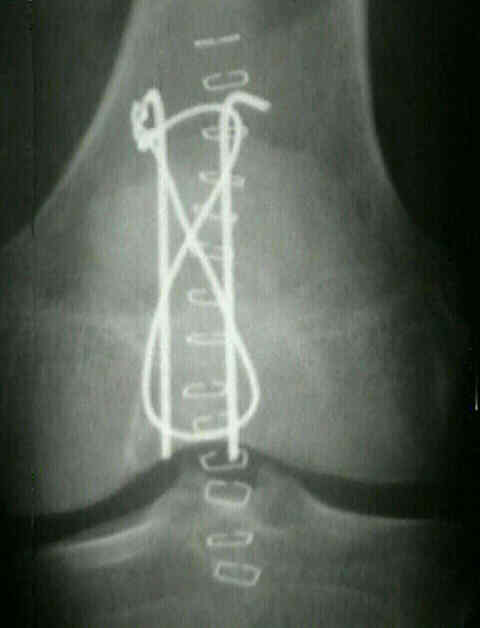
- tension band technique:
- partial patellectomy
- consider advancement of the fibers of the vastus medialis over the repair site;
- reenforment of the repair may be achieved by turning down half the thickness
of the rectus tendon;
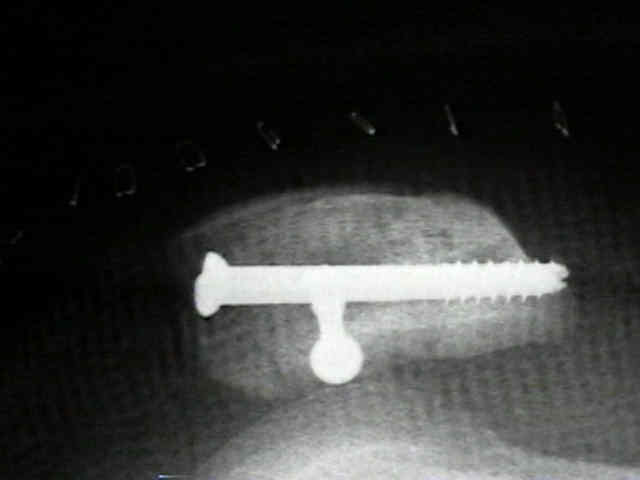
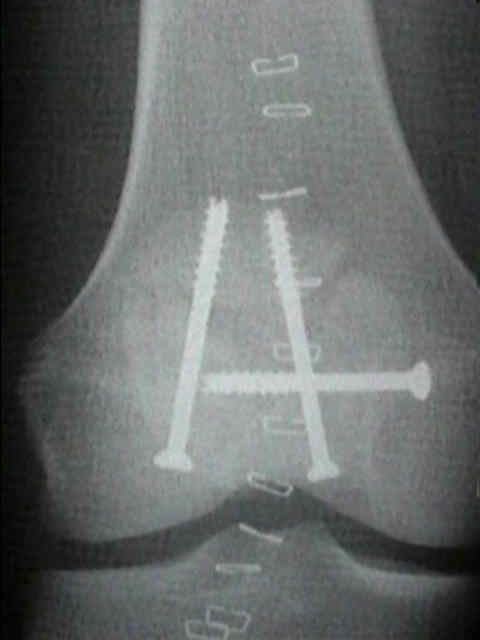
- screw fixation:
- Biomechanical evaluation of current patella fracture fixation techniques
- cannulated screw fixation w/ tension band: (theory of tension band)



- [Proper and improper tension band fixation exemplified by patellar fracture]
- FiberWire is superior in strength to stainless steel wire for tension band fixation of transverse patellar fractures
- A new and effective tension-band braided polyester suture technique for transverse patellar fracture fixation
- ORIF of displaced patella inferior pole fractures with anterior tension band wiring through cannulated screws.
- ORIF of displaced transverse patella fractures with figure-eight wiring through parallel cannulated compression screws.
- Cannulated Screw and Cable are Superior to Modified Tension Band in the Treatment of Transverse Patella Fractures
- Post Op Care:
- joint in immobilized in 40-60 deg flexion for 2-3 days & extremity is elevated;
- on POD 4, begin ROM exercises;
- ROM is required to enhance cartilage healing and for physiologic frx compression thru figure of 8 apparatus;
- consider using prone hangs: patient lies in the prone position and flexes and extends the knee;
- these exercises avoid active knee extension and avoid excessive stress at the fracture site;
- wt bearing is allowed at 4-6 wks;
- outcomes:
- Outcomes After Operative Fixation of Complete Articular Patellar Fractures: Assessment of Functional Impairment
- Complications of Patella Fracture:
- infection (which communicates with the knee joint)
- loss of reduction
- failure of internal fixation
- avascular necrosis:
- patella has two main areas of blood supply (see blood supply)
- one penetrates middle third of anterior surface, & other enters at lower pole behind patellar ligament;
- delayed union
- non union
- delayed union is recognized by failure of trabeculae to bridge between patellar frags, as noted on x-rays 2 mo after injury;
- typically frxs will have > 2 mm of gap between fracture fragments;
- non union can be diagnosed after 3-4 months of treatment;
- occassionally elderly patients tolerate nonunions well, however, younger patients do not tolerate nonunion;
- nonunion is most common in transverse frxs, but may be seen in comminuted frxs that have failed to acheive internal fixation;
- partial or total patellectomy is preferred in most pts w/ non union, esp if disuse osteoporosis or AVN is present
- malunion
- chondromalacia
- traumatic arthritis of the patellofemoral joint
- quadriceps weakness
- extensor lag
- avascular necrosis of the polar fragments
- arthrofibrosis of the knee joint
Fracture of the patella treated by open reduction and external compressive skeletal fixation.
Efficacy of various forms of fixation of transverse fractures of the patella.
Indications and results of nonoperative treatment of patellar fractures.
Transverse fractures of the patella.
Blood supply of the human patella. Its relation to ischaemic necrosis after fracture.
Implant removal following surgical stabilization of patella fracture
Early complications in the operative treatment of patella fractures
Treatment of delayed and nonunion of the patella
...............................................................................................................................................................................................................................................................................................