

- See: Total Hip Replacement Menu:
- Discussion:
- natural history of DDH:
- acetabular rim syndrome:
- results from dysplastic hip, which stresses the labrum, resulting in labral degeneration;
- hip arthroscopy and debridement in these patients may provide the patient w/ a few additional years before THR is required;
- THR preoperative considerations:
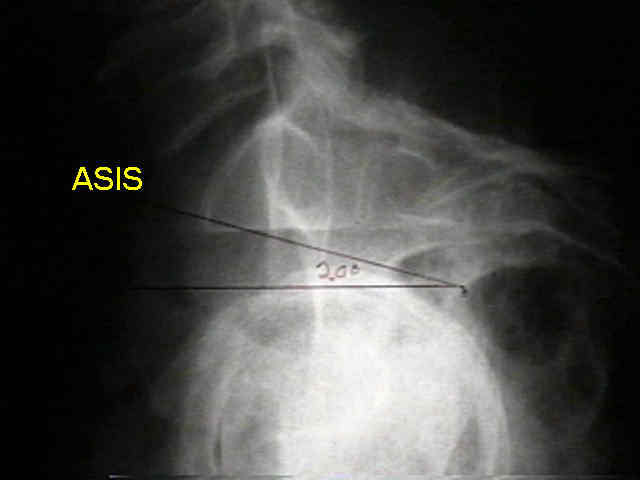
- center edge angle
- note that revision THR shares many of the problems encountered with the dysplastic hip;
- when the hip is located in the native acetabulum, the acetabulum is often shallow, abducted, and significantly anteverted;
- soft tissue adaptive changes may include hyperlordosis, adduction contracture, and leg length descrepancy;
- risk of component dislocation may be especially prevalent in these patients;
- references:
- Three Patterns of Acetabular Deficiency Are Common in Young Adult Patients With Acetabular Dysplasia
- considerations for alternative procedures:
- in patients less than 45-50 yrs, alternative procedures should always be considered;
- pelvic osteotomy in DDH: (Chiari, Shelf, Ganz, and Penberton osteotomies are considered);
- femoral osteotomy in DDH
- Crowe Classification: (Paprosky classification)
- Technical Considerations for the Acetabulum:

- acetabular component menu:
- anatomy:
- How Are Dysplastic Hips Different? A Three-dimensional CT Study
- cotyloplasty technique / medial protrusio technique:
- bone grafting for THR:
- autogenous femoral head grafting for anterolateral acetabular deficiency:
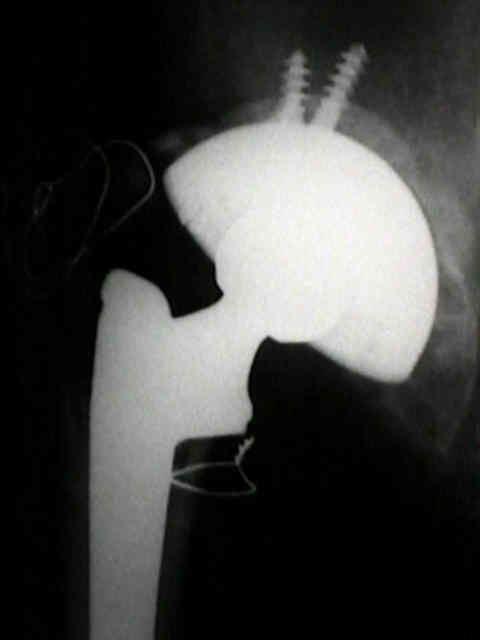
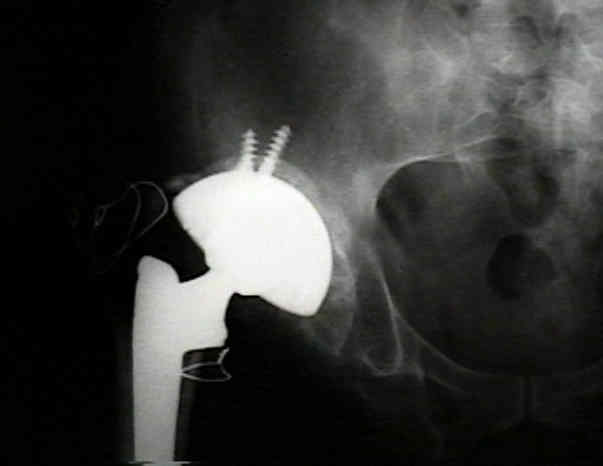
- Spangehl et al: 44 hips in 35 patients w/ DDH were treated w/ THR with press fit cup fixed with screws
and femoral head graft;
- 4 acetabular components were revised: 2 due to polyethylene wear & 1 due to aseptic loosening,
1 due tobecause frx of acetabular shell;
- 43 of the 44 hips had no radiographic evidence of resorption of the graft or had radiographic
evidence of resorption limited to the nonstressed area of the graft lateral to the edge of the cup;
- references:
- Uncemented acetabular components with bulk femoral head autograft for acetabular reconstruction in developmental dysplasia of the hip: results at five to twelve years.
- Total hip replacement with the CLS expansion shell and a structural femoral head autograft for patients with congenital hip disease.
- Total hip arthroplasty with cement and without acetabular bone graft for severe hip dysplasia. A concise follow-up, at a minimum of twenty years, of a previous report
- Femoral head autografting with total hip arthroplasty for lateral acetabular dysplasia. A 12-year experience.
- Autogenous bone grafts from the femoral head for the treatment of acetabular deficiency in primary total hip arthroplasty with cement, long-term results.
- acetabular component position:
- key question is whether to place acetabulum cup in an anatomic (inferior) or a non-anatomic (superior) position;
- where there is the greatest bone stock so that the osseous coverage of the acetabulum can be optimized;
- how much shortening of the femur is required;
- up to 4 cm of lengthening is usually safe;
- it is impotant to template how much femoral shortening will be required to avoid maximal lengthening;
- note the tension on the nerve both at the beginning and the end of the case;
- anatomic position:
- non-anatomic positioning: (high hip center)
- references:
- Outcome of revision hip arthroplasty in patients with a previous total hip replacement for developmental dysplasia of the hip.
- Dislocation After Total Hip Arthroplasty Among Patients With Developmental Dysplasia of the Hip
- Cementless Acetabular Reconstruction and Structural Bone-Grafting in Dysplastic Hips.
- Cementless Acetabular Reconstruction and Structural Bone-Grafting in Dysplastic Hips. Surgical Technique
- THR for developmental dysplasia of the hip with more than 30% lateral uncoverage of uncemented acetabular components
- Technical Considerations of the Femur in DDH:

- significant anteversion of the femoral neck;
- w/ more than 40 deg of anteversion, consider derotation with subtrochanteric osteotomy;
- femoral medullary canal is narrow;
- this may be managed by splitting the proximal 8-10 cm of the femoral shaft both anteriorly and
posteriorly and then establishing rigid fixation after the stem has been inserted;
- medullary canal may be distorted from previous osteotomies (in which case a subtrochanteric
osteotomy may be required);
- short femoral neck;
- distorsion of proximal femoral shape from previous osteotomies;
- leg length descrepancy:
- significant leg length descrepancy is seen in high dislocations;
- attempts at leg length equalization may result in sciatic neuropraxia;
- as pointed out by, Kavanagh et al 1991, no patients that had leg lengthing of less than 4 cm developed a palsy;
- when lengthening was more than 4 cm, 28% of patients developed a sciatic nerve palsy;
- ref: Predicting leg-length change after total hip arthroplasty by measuring preoperative hip flexion under general anaesthesia.
- femoral shortening
- may be performed by proximal shortening or by subtroch osteotomy (step cut or oblique subtrochanteric osteotomy);
- proximal shortening is not be performed distal to the lesser trochanter because there is not be enough of a
metaphyseal flare left to support the femoral implant;
- references:
- Total hip arthroplasty with shortening subtrochanteric osteotomy in Crowe type-IV developmental dysplasia: surgical technique.
- Double-chevron subtrochanteric shortening derotational femoral osteotomy combined with total hip arthroplasty for the treatment of complete congenital dislocation of the hip in the adult. Preliminary report and description of a new surgical technique.
- Total Hip Arthroplasty With Shortening Osteotomy in Congenital Major Hip Dislocation Sequelae
- Subtrochanteric shortening osteotomy combined with cemented total hip arthroplasty for Crowe group IV hips
- Transverse Subtrochanteric Shortening Osteotomy During Cementless Total Hip Arthroplasty in Crowe Type-III or IV Developmental Dysplasia
- trochanteric osteotomy:


Coxarthrosis after congenital dysplasia. Treatment by total hip arthroplasty without acetabular bone-grafting.
Total hip arthroplasty in high congenital dislocation. 21 hips with minimum five-year follow-up.
Total hip replacement for coxarthrosis secondary to congenital dysplasia and dislocation of the hip. Long term results.
Total Hip Arthroplasty for Congenital Hip Disease.