

- See:
- radiographic templating of femoral neck cut
- femoral component offset
- Discussion:
- femoral neck cut will influence leg length, caput collum diaphysis (CCD) angle, and offset;
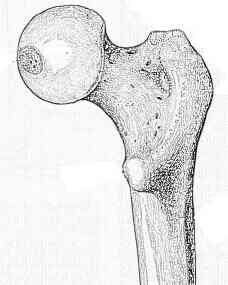
- base of the femoral neck ("the shoulder") is used as a reference for appropriate level of osteotomy;
- Exposure:
- blunt Homan retractors are placed around the femoral neck, w/ one broad Homan retractor placed underneath the neck
and one sharp Homan placed just distal to the lesser trochanter inorder to deliver the proximal femur into the wound;
- avoid excessive retraction of the homan under the lesser trochanter as this can impinge on the sciatic nerve;
- keep leg flexed, internally rotated, and horizontal to ground;
- remove soft tissue structures of the lateral neck and off the medial side of the greater trochanter;
- a roungeur is then used to remove bone a the base of the medial greater trochanter just anterior to the piriformis fossa;
- a clear view of the lateral neck is obtained so that the stem is not placed in varus;
- Femoral Neck Cut:
- measure verticle and horizontal offset from the tip of the greater trochanter to the center of the femoral head and compare to preoperative radiographic templates;
- mark the level and angle of the proposed osteotomy of the femoral neck;
- make the osteotomy 2 mm higher than preoperative templating;
- tendency is to cut neck so that the anterior cortex is longer than posterior cortex, which will tend to produce retroversion of the component;
- ensure that anterior cortex is cut more distal than posterior cortex, so that during broaching there will not be false impression that
the canal needs additional broaching;
- incorrect resection Level:
- high resection level:
- a restion level that is too high would yield excessive space medially in the proximal canal, leading one to believe that the stem is too small;
- tends to cause varus stem placement;
- tends to cause high placement of head;
- low resecton level:
- a low resection level would give the impression that stem is too large;
- causes incomplete seating
- may cause valgus stem placement
- may cause low placement of head;
- appropriate resection level:
- even if the femoral neck osteotomy is made at the correct templated level, there is no guarantee that this allows for optimal
stem fit and allows for optimal soft tissue balance as well as restoration of horizontal and verticle offset;
- note that with press fit stems there will often be a choice between a stem that is slightly too large vs slight too small;
- in this situation, the large stem will sit proud (missing the femoral neck osteotomy by several mm) whereas the smaller
stem will have to be impacted to a lower level inorder to obtain an adequate press fit;
- final trial reduction:
- the final trial reduction made after the acetabular component is set in place will help determine final optimal neck level;
- in some cases, there will be good stability but excessive soft tissue tension (absence of shuck test), which can be managed by lowering the femoral
neck resection level, and then again performing a trial reduction;
- because most femoral stem necks are now 130 to 137 deg, an increase in femoral neck length increases the offset more than leg length;
- if femoral neck resection is < nl, offset can therefore be increased by using longer neck w/o significant increase in leg length
Effect of neck resection on torsional stability of cementless total hip replacement.
Fixation of the modular total hip femoral component in cementless total hip arthroplasty.
Effect of a cooled saw blade on prosthesis fixation. Randomized radiostereometry of 33 knee cases.
On the problem of heat generation in bone cutting. Studies on the effects on liquid cooling.
Histopathology of Femoral Head Donations: A Retrospective Review of 6161 Cases
Femoral Neck Cut Level Affects Positioning of Modular Short-Stem Implant
Preserving the femoral neck in hip replacement: a concept for the future?