


- Discussion:

- screw is threaded at both ends and can be countersunk beneath articular surface, obviating the need for
removal after frx has healed;
- it is designed to achieve compression by use of a differential thread-pitch between its proximal & distal ends,
and it has guiding jig that maintains reduction & interfragmentary compression during insertion;
- disadvantages:
- interfragmentary compressive forces generated by Herbert screw are less than those associated with
conventional screws;
- most of the interfragmentary compression obtained results from the Herbert screw jig and not the
screw itself;
- indications for surgery:
- main indication is an unstable scaphoid frx as seen on x-ray or CT;
- displacment > 1 mm;
- radiolunate angle > 15 degrees;
- scapholunate > 60 degrees;
- indicated for patients w/ delayed unions or non unions of scaphoid waist;






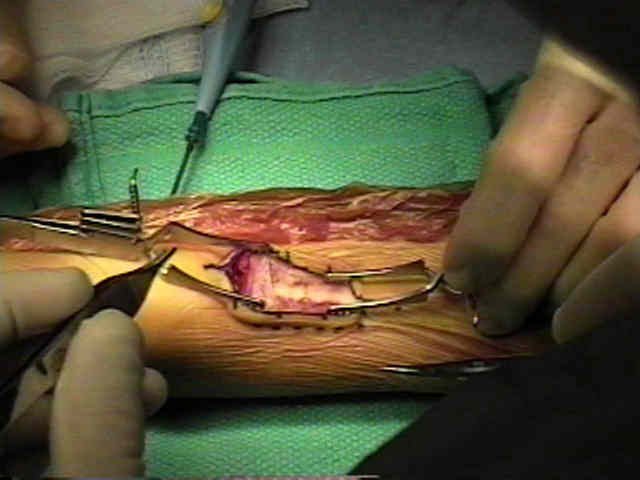
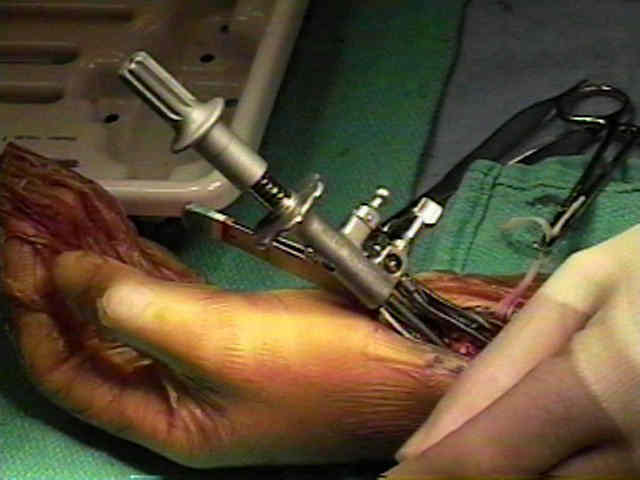
- Partial Removal of Distal Trapezium:


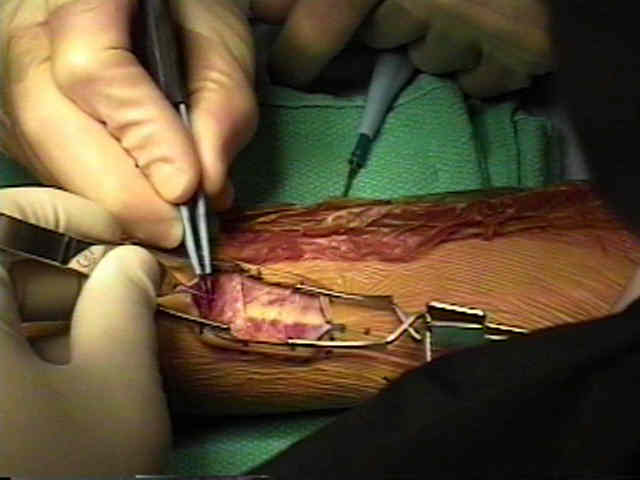
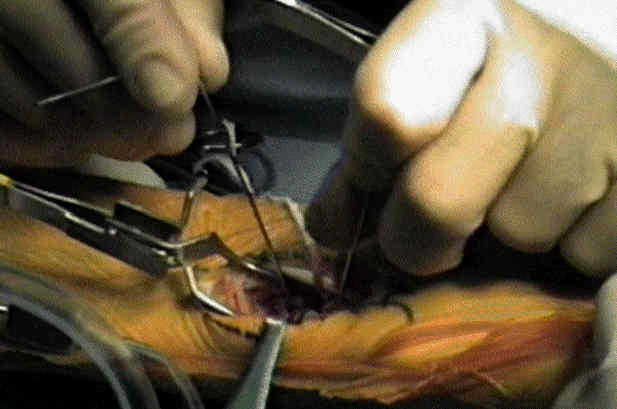
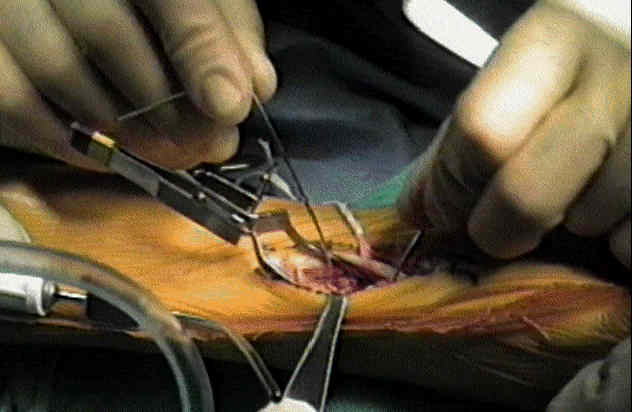
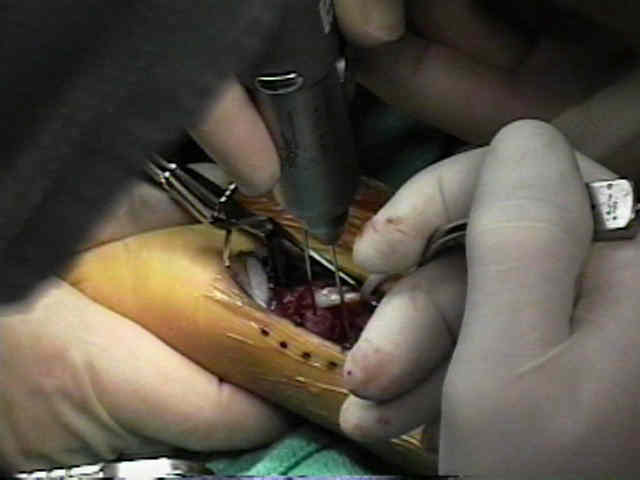
- Frx Reduction:
- frx is carefully reduced & held by passing K wire across bone in such way that it will not interfere w/ placement of jig and screw.
- alternatively, the cannulated Herbert screw can be used which does not require use of the jig;
- the K wire holds the reduction and serves as a guide for the screw;
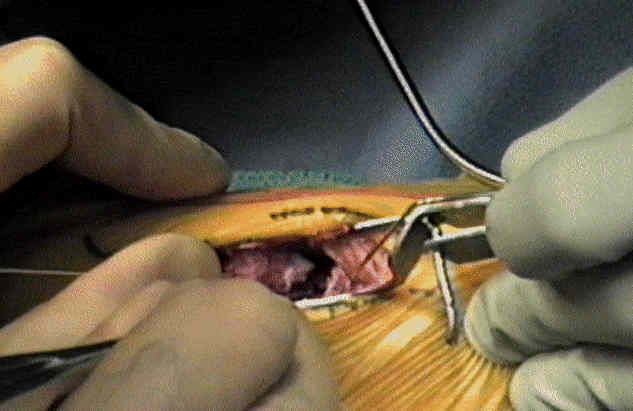
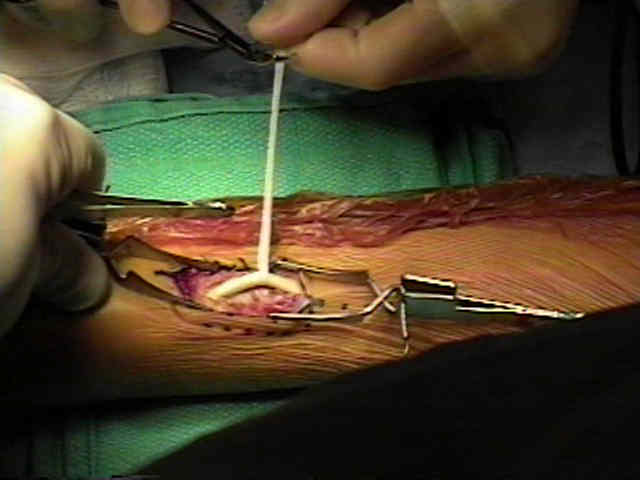
- w/ comminuted frx, loose fragments are removed and sufficient bone graft is inserted to provide stability under compression w/o
deformity;
- w/ a well alinged non union, bone graft may consist of cancellous chips;
- w/ a malaligned non union which requires reduction, bone graft should be a cortico-cancellous piece shaped to fill the defect;
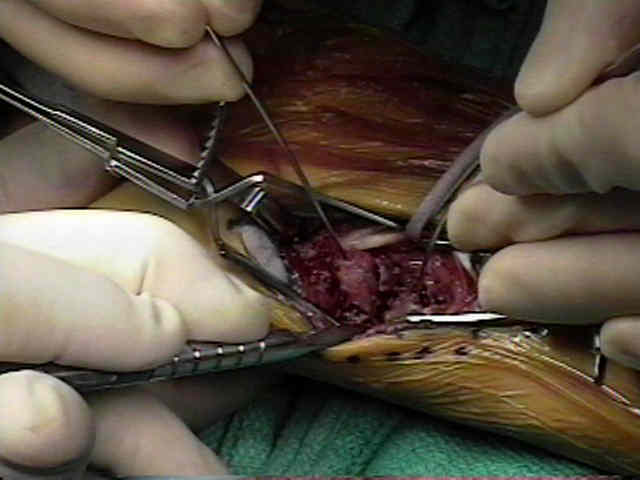
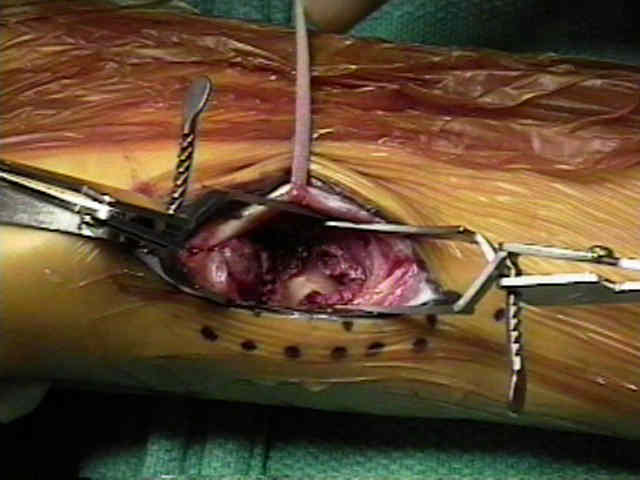
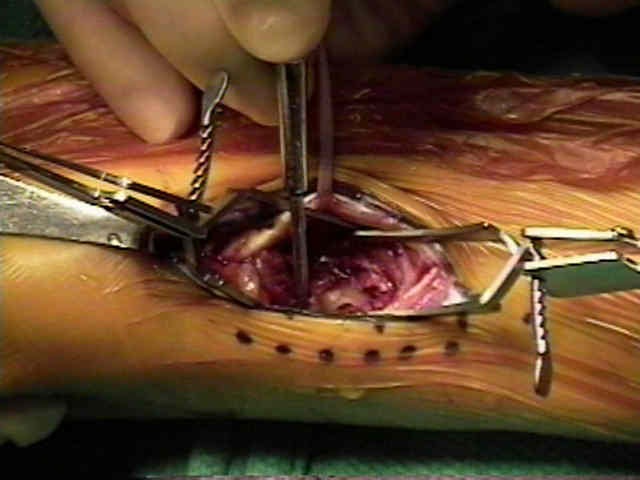
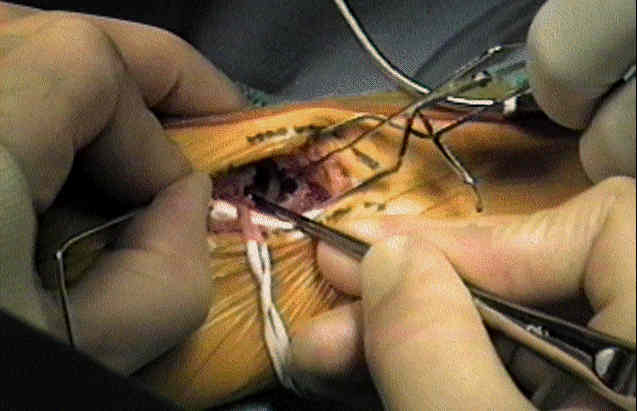
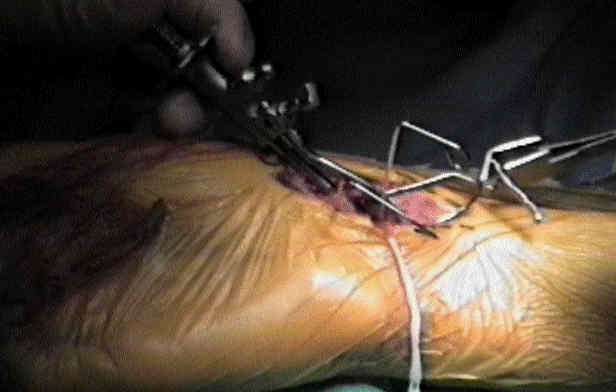
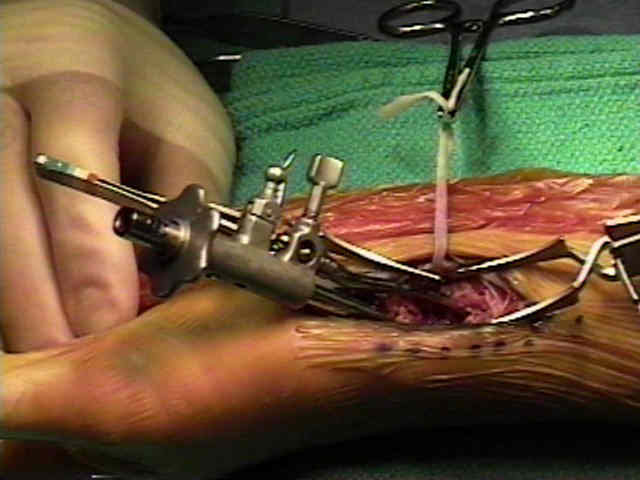
- Jig Application: (optional)
- drill guide is placed across the distal pole, and the blade tip is placed across the proximal pole;
- wherever possible, jig should be applied in such a way that screw will be perpendicular to fracture;
- if obliquity of frx line makes this impossible, supplementary K wire fixation should be used to prevent shearing displacement
under compression;
- if there is difficulty apply the jig, consider removing a small portionof the trapezium;
- the jig must be placed more dorsal than expected inorder to avoid creating a humpback deformity;
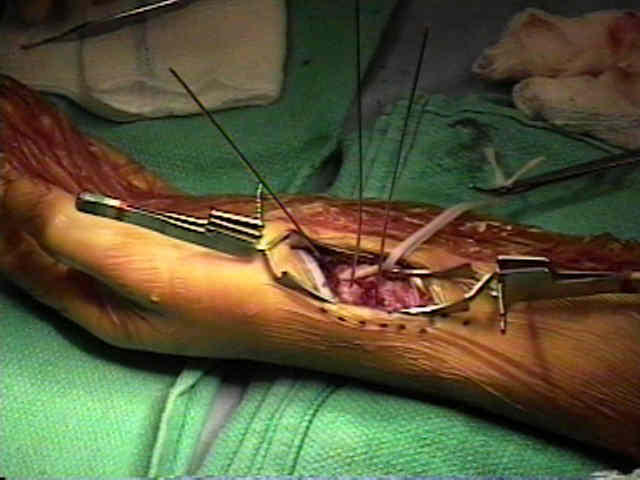
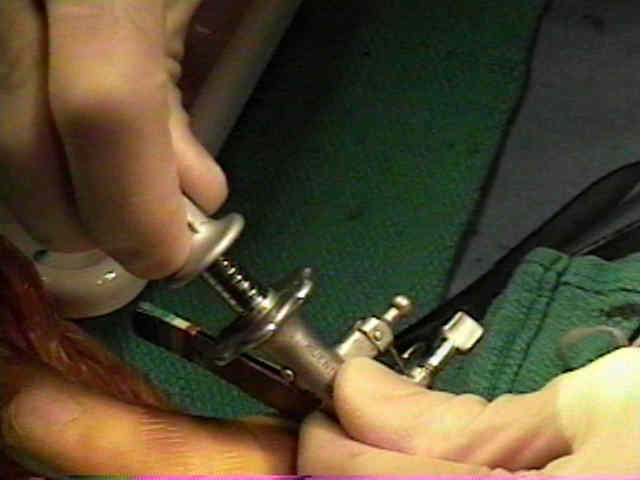
- frx site is compressed by jig prior to screw placement;
- as jig is compressed ensure that there is not excessive volar compression which will cause a humpback deformity;
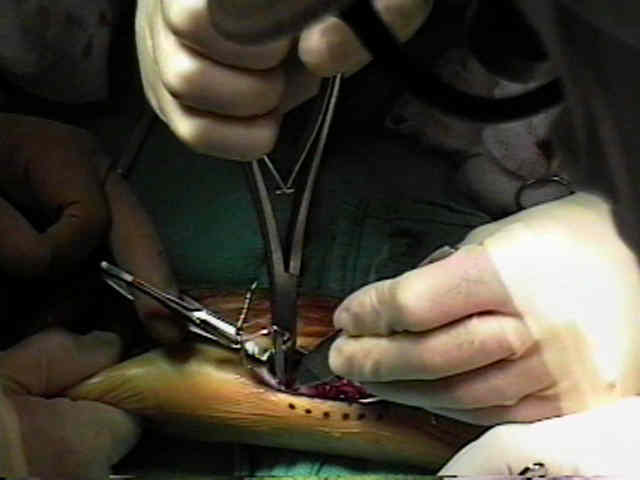
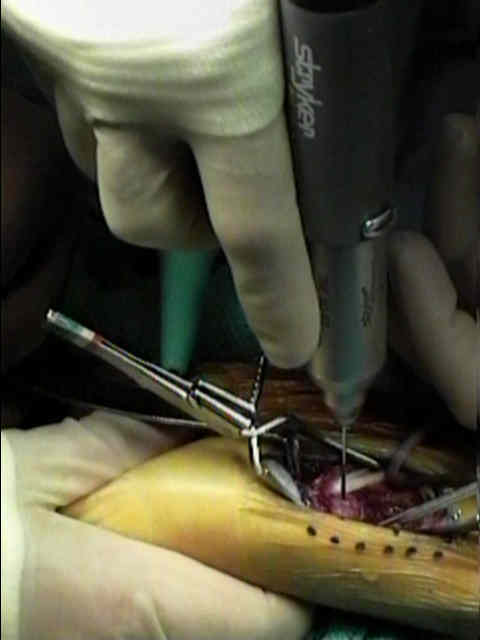
- measure screw size, off of calibrated guide;
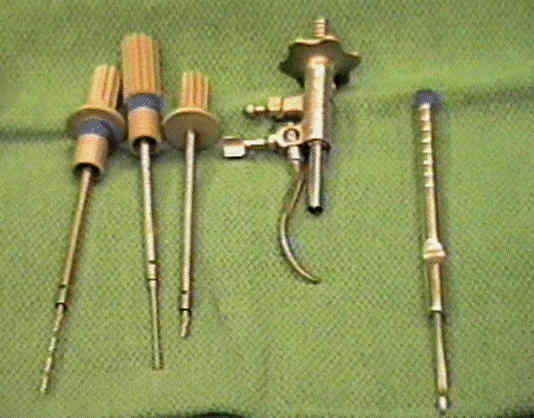
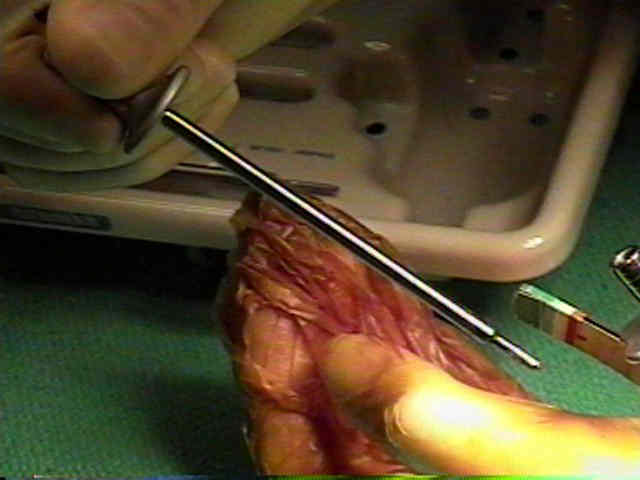
- insert pilot drill for trailing edge of screw;
- long drill is inserted for leading end of screw;
- tap for leading thread (trailing end is self tapping);
- insert screw through jig;








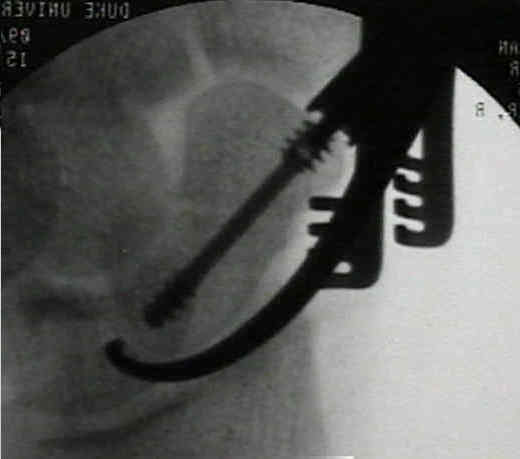
- Final Radiographic Appearance:



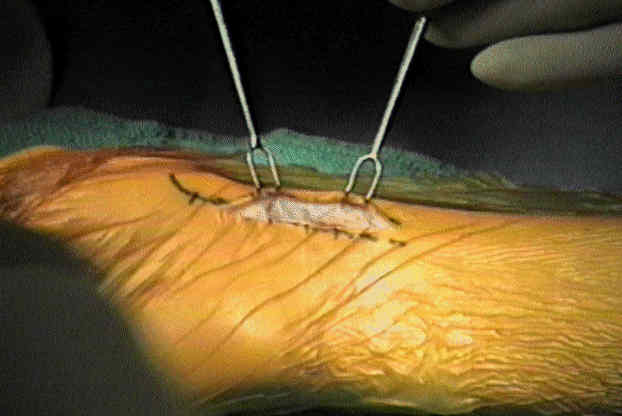
- Post Op Care:
- even w/ Herbert screw fixation many recommend that immobilization be continued in short thumb-spica cast until there is evidence
of frx union
Management of the Fractured Scaphoid Using a New Bone Screw.
The Herbert screw for scaphoid fractures. A multicentre study.
Technical factors related to Herbert screw fixation.
Two modifications for insertion of the Herbert screw in the fractured scaphoid.
Internal fixation of scaphoid injuries using the Herbert screw through a dorsal approach.
Problem Disorders of the Wrist--Symposium: Use of the Herbert Bone Screw in Surgery of the Wrist.