

CPT Daniel Stinner, M.D.
B. Define early management of extremity burns
I. Early Wound Management
A. Introduction
1. not necessary to perform immediately, but should be done within first 24 hours
2. ensure patient receives adequate pain medicine, as wound care can be very painful
B. Goal
1. set conditions for wound closure
2. prevent burn wound sepsis – combat burns and burns in austere environment are contaminated, dirty wounds
C. Steps
1. best performed in warm, clean environment with anesthesia support
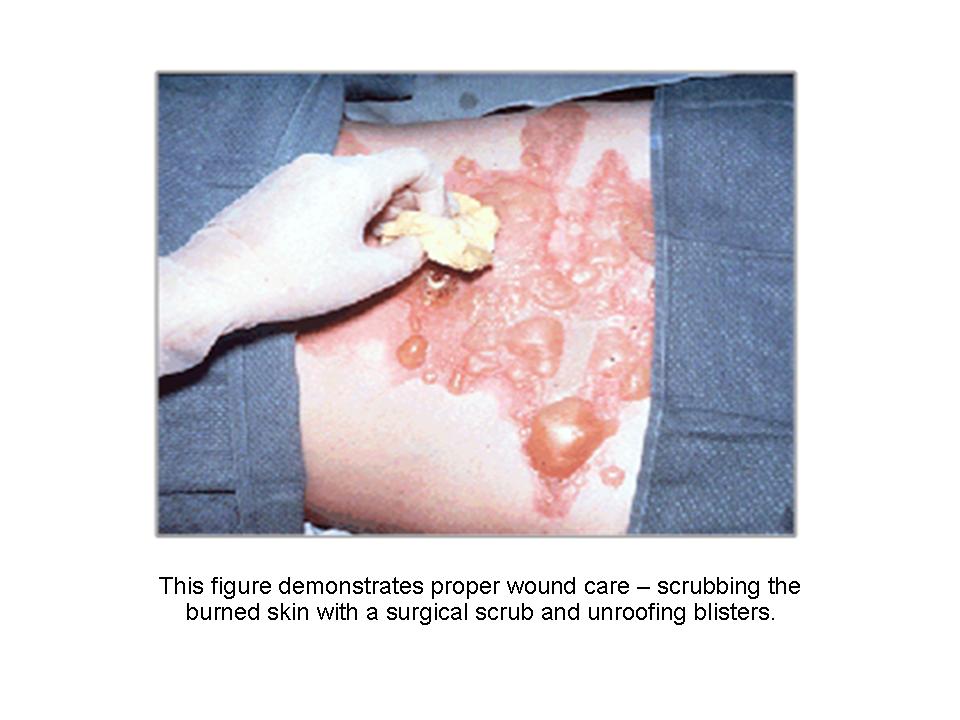
2. chlorhexidene gluconate (Hibiclens, Zeneca Pharmaceuticals, Wilmington, DE) cleansing
a. scrub all exposed skin with surgical antimicrobial cleansing solution
b. saline should be used for face due to irritation that can be caused by cleansing solutions (see figure 6)
{kind=link}
3. debridement – all foreign bodies must be removed and blisters unroofed
4. topical antimicrobial agents – various agents available with different frequencies of application
a. providers in the field should simply cover the wounds with dressings and not apply topical ointments or burn creams5
b. common examples:1% silver sulfadiazine (Silvadene, Monarch Pharmaceuticals, Bristol, TN or 11.1% mafenide acetate (Sulfamylon, Bertek Pharmaceuticals, Morgantown, WV), applied thick (1/16 to 1/8 inch thick)
c. typically applied twice daily, but depends on topical agent used
5. dry, bulky dressings – applied to protect burned skin from environment and help minimize fluid losses through exposed skin
a. silver-nylon dressings covered by gauze are ideal5
6. cold water treatment has been shown in animal studies to increase survival for large TBSA burns4
II. Special Considerations
A. Large, open wounds in the area of the burn
1. Debride as normally would be done
2. Leave these wounds open
3. Use negative pressure/vacuum assisted closure devices for temporary coverage
B. Extremity burn with fracture – can pose significant challenge, initial management in austere environment similar to in tertiary medical center
1. reduce and immobilize fracture
a. skeletal traction – while common practice years ago and may be only option in austere environment, not ideal for patient transportation
b. splint – typically easy to construct, but in patient with burn injury to same extremity, access to wound needed for daily wound care, also burned extremities tend to weep
i. may be ideal for stable fractures and small TBSA burns
ii. not typically used for unstable fractures with larger TBSA burns
iii. ensure circumferential casts or splints bivalved to accommodate potential edema
c. external fixation
i. better suited for patient transportation in austere environment and allows access to large wounds for daily wound care
ii. fixation pin placement
(A). preferred placement is through unburned skin
(B). alternatively, pins can be placed through burn wound
2. check pulse before and after reduction
3. prior to prolonged transport, consider escharotomy – after escharotomy, document return of pulse and continue to follow
C. Electrical injury
1. high voltage (greater than 1,000 volts) can cause muscle damage, which does not always correlate with skin injury
2. muscle cells leak: myoglobin, K+, and Phos2-
a. acute renal failure
b. cardiac dysrhythmias
3. look for focal extremity entry and exit points
4. management: aggressive fluid and electrolyte management
5. monitor extremity exam and consider fasciotomies if clinical concern
D. Chemical burns
1. initial treatment – remove offending agent
2. brush away dry material before copious water lavage
3. with alkali burns, lavage may need to be continued for hours
4. resuscitate as in thermal burn
E. White phosphorus burn
1. most of cutaneous injury is due to ignition of clothing, treat as conventional burn
2. remove all fragments that may reignite upon contact with air, prevent with removal and cover with saline-soaked gauze
3. UV light can help identify particles that need to be removed
4. treat and resuscitate as thermal burn once all particles/fragments removed from wound
F. Corneal abrasion
1. can lead to full-thickness ulceration and blindness
2. gentamicin or quinolone antibiotic ointment every 4 hours, alternating with erythromycin ointment every 4 hours
C. Demonstrate the proper technique for escharotomy
I. Surgical Technique: Escharotomy (see figure 7)
{kind=link}
A. Introduction
1. typically performed at bedside under sterile condition with IV sedation using electrocautery
2. can also be performed in operating room if immediate access available
3. electrocautery has added benefit of haemostatic control, but if unavailable, scalpel can be used
4. general principle
a. to make surgical incisions through burned eschar to allow expansion of underlying tissues
b. if perfusion does not return following escharotomy, fasciotomies are indicated
B. Chest escharotomy
1. in circumferential chest burns, chest wall expansion may be restricted, resulting in decreased ventilation
2. chest escharotomy can be performed to improve ventilation
a. lateral incisions are made on both sides of chest
b. these incisions are connected via transverse or inverted V-shaped incision just below costal margin
c. goal is to separate thorax from abdomen effectively and improve chest wall expansion (see figure 8)
.jpg){kind=link}
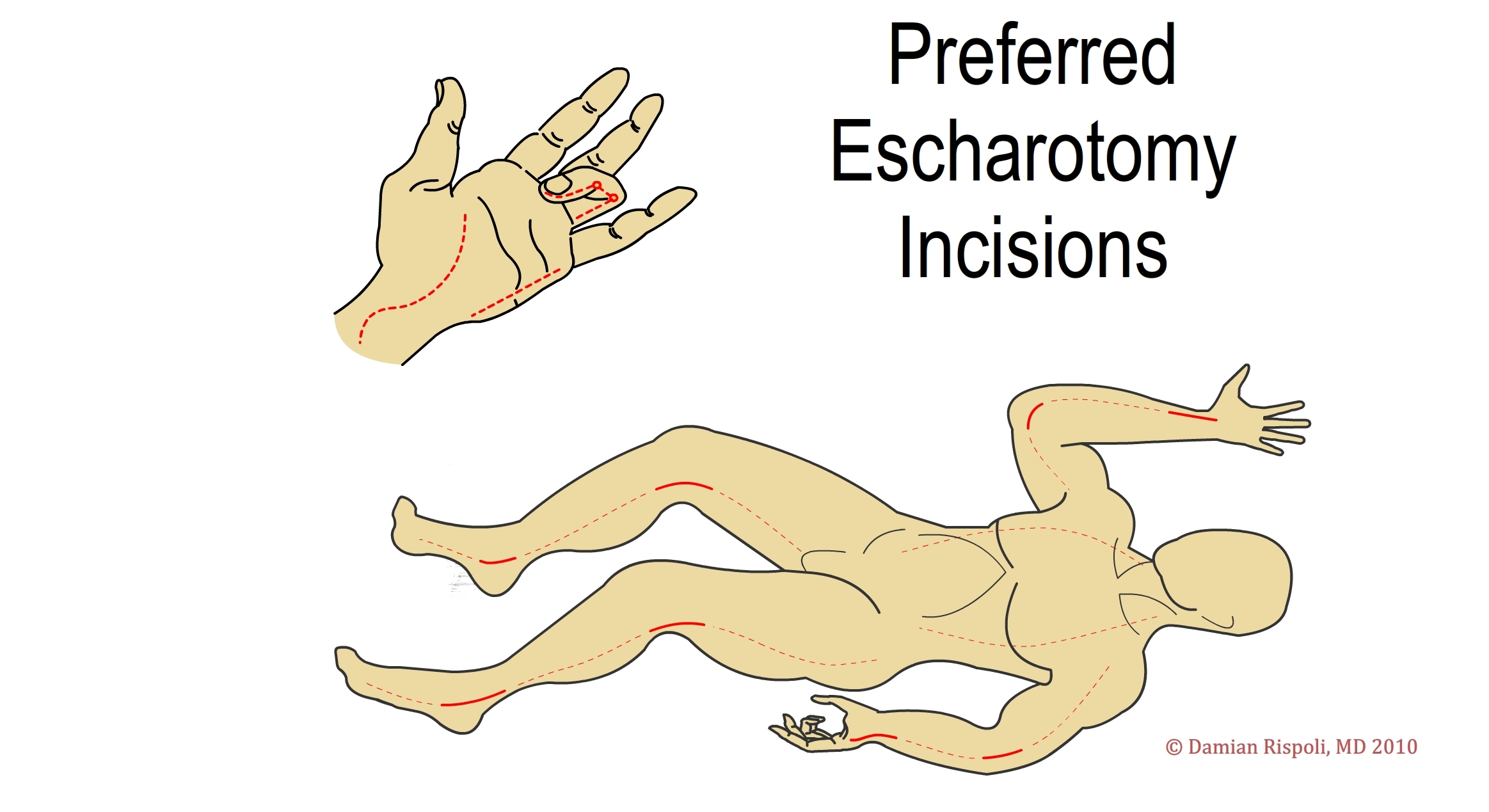
C. Extremity escharotomy
1. full-thickness incisions along medial and lateral midaxial lines should be made (see figure 9), ideally, escharotomy incisions performed through same skin incisions that could be used later for fasciotomies, if indicated (see figure 10)
.jpg){kind=link}
.jpg){kind=link}
2. escharotomies should be carried to just beyond the area of full-thickness burn
a. when in doubt, make incision longer rather than shorter because burns tend to evolve during period immediately following the burn
b. special considerations for upper extremity escharotomies
c. know your anatomy – watch for superficial structures
i. at level of wrist, watch for superficial branch of radial nerve along radial side of wrist
ii. (at level of elbow, watch for ulnar nerve at level of medial epicondyle
d. digital escharotomies can be performed along midaxial line between neurovascular bundle and extensor apparatus; the ideal side to perform escharotomy allows for preservation of pinch
i. thumb – radial incision
ii. index finger, middle finger, ring finger, small finger – ulnar incisions
e. hand escharotomies can be performed over the index finger metacarpal and ring finger metacarpal; if this release is inadequate, incisions can be converted to fasciotomies (see hand fasciotomies section)
f. carpal tunnel releases may also be required to achieve adequate decompression of hand
g. children more prone to compartment syndromes and distal tip necrosis due to smaller cross-sectional area, but performing digital escharotomies in children remains controversial
II. Injuries Requiring Burn Unit Care
A. Introduction
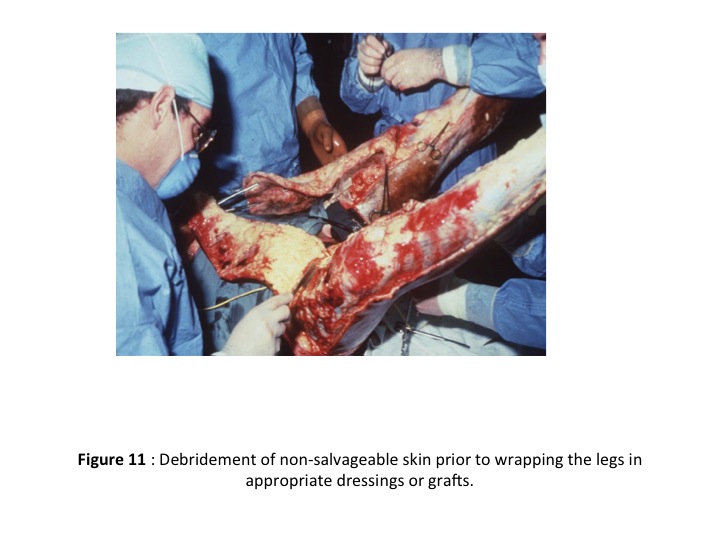
1. in austere environment, appropriate facilities or resources may not be available for definitive treatment (see Figures 11 and 12)
{kind=link}
.jpg){kind=link}
2. if available, plan early and begin preparing patient for transfer following stabilization
B. Committee on Trauma of the American College of Surgeons recommends referral to burn unit if following criteria are met3
1. inhalation injury
2. partial-thickness burns greater than 10% TBSA
3. full-thickness (third degree) burns in any age group
4. burns that involve face, hands, feet, genitalia, perineum, or major points
5. electrical burns, including lightening injury
6. chemical burns
7. burn injuries in casualties with preexisting medical conditions that may complicate management, prolong recovery, or affect mortality
8. any casualties with burns and concomitant trauma in which the burn injury poses the greatest risk of morbidity or mortality; if trauma poses greater immediate risk, patient may be initially stabilized in trauma center prior to transfer to burn unit
9. burned children in hospital without qualified personnel or equipment for care of children
10. burn injury in casualties who will require special social, emotional, or long-term rehabilitative intervention
References
1. Potin M, Sénéchaud C, Carsin H, et al. Mass casualty incidents with multiple burn victims: rationale for a Swiss burn plan. Burns. 2010;36(6):741-750.
2. Owens BD, Kraugh JF Jr, Macaitis J, et al. Characterization of extremity wounds in Operation Iraqi Freedom and Operation Enduring Freedom. J Orthop Trauma. 2007;21:254-257
3. American College of Surgeons Committee on Trauma: Resources for optimal care of the injured patient: 2006, Chicago, 2006, ACS.
4. Cuttle L, Pearn J, McMillan JR, Kimble RM. A review of first aid treatments for burn injuries. Burns. 2009;35:768-775
5. White CE, Renz EM. Advances in surgical care: Management of severe burn injury. Critical Care Medicine. 2008;36;S318-324.
Additional Resources
Alverarado R, Chung KK, Cancio LC, et al. Burn resuscitation. Burns. 2009;35(1):4-14.
American College of Surgeons Committee on Trauma: Resources for optimal care of the injured patient: 2006, Chicago, 2006, ACS.
Herndon DN, ed. Total Burn Care. Philadelphia, PA: Elsevier, 2007.
NAEMT. PHTLS: Prehospital Trauma Life Support, Military Edition. St. Louis, MO: Elsevier, 2010.
Szul ADL, ed. Emergency War Surgery, Washington, DC: Walter Reed Army Medical Center Borden Institute, 2004.
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, Department of Defense or the U.S. Government.
Materials and support for The Disaster Preparedness Toolbox is provided by Lt Col. Ky Kobayashi, MD and Col. Benjamin Kam, MD.