

CPT Jeanne Patzkowski, M.D.
CPT Chad Krueger, M.D.
B. Define the initial management, resuscitation, and stabilization of spine injuries with associated neurological injuries
IV. Stabilization
A. Maintain rigid spinal immobilization until mechanical instability has been ruled out
1. may need CT scan to evaluate entire spine completely
2. majority of gunshot wounds to spine are mechanically stable in patients with normal neurologic exam
a. if damage limited to one column of spine, no particular immobilization is needed
b. if two or more columns damaged, spinal precautions and immobilization should be continued until definitive fixation at echelon IV/V facility
B. Immobilization
1. rigid cervical collar
a. may also consider supplementing with bilateral neck supports (sand bags, IV fluid bags, etc.), and taping across forehead to backboard
b. soft collars are insufficient for unstable C-spine injuries
2. rigid backboard
a. facilitates logroll maneuver
b. pressure necrosis may develop within two hours
c. discontinue once mechanically unstable spinal injury has been ruled out
C. Reduction
1. axial traction may be performed at echelon III facilities and higher
a. must rule out atlanto-occipital dissociation before applying traction
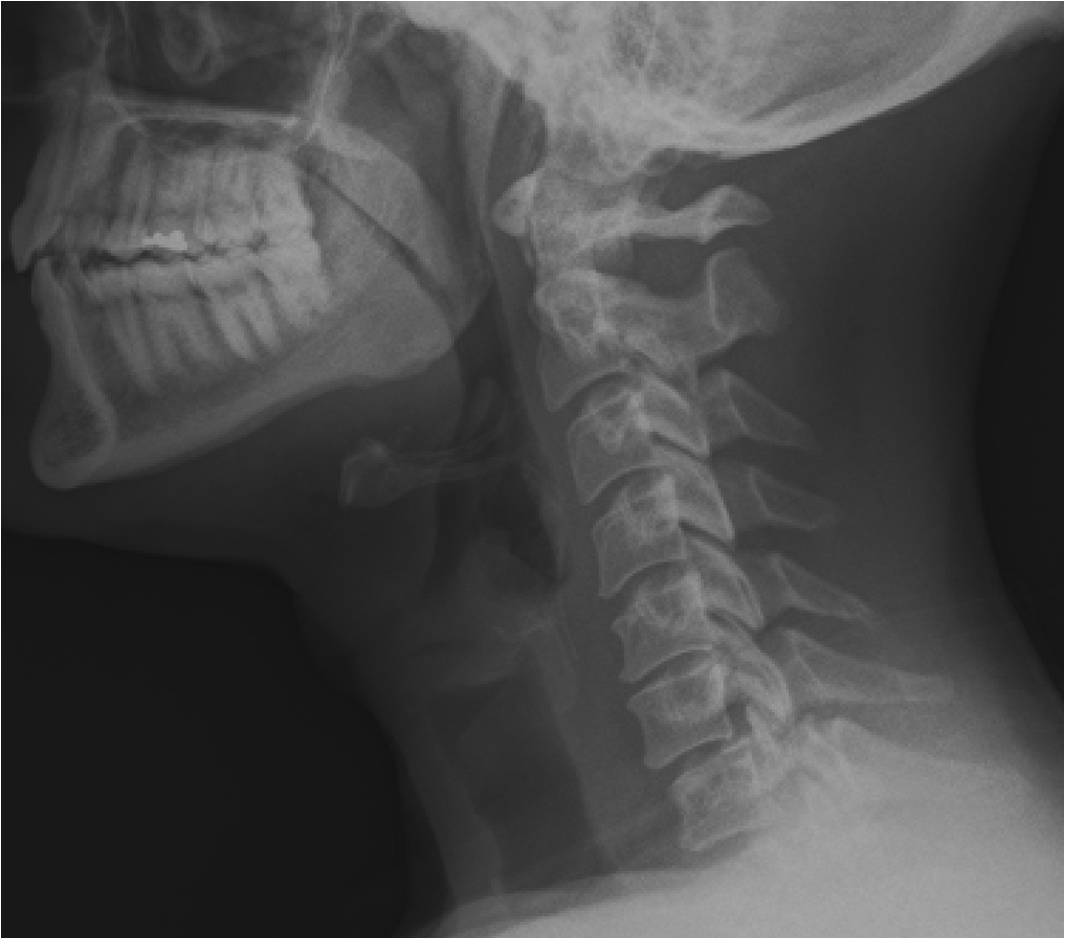
i. may be seen on lateral C-spine plain films
ii. most reliably detected on CT scan
b. perform only in awake patients
c. serial radiographs and neurologic exams
d. stop attempt at reduction for:
i. development of new neurologic deficit
ii. one cm distraction of a disk space
e. post reduction radiographs
2. Gardner-Wells tongs
a. simple
b. do not require an assistant to place
c. allow axial traction
d. do not control rotation, flexion or extension
3. halo ring
a. more complicated
b. requires assistant to place
c. allows axial traction
d. improved control of rotation, flexio, and extension
D. Surgery
1. emergency surgery indicated only for incomplete spinal cord injury with progressive neurologic deficit
a. must ensure meticulous dural repair with tight closure of muscle, fascia, and skin
b. if dura cannot be closed, ensure watertight skin closure
c. progressive neurologic deficit is only indication to remove bullet or fragment in disk space or spinal canal emergently (echelon III); otherwise surgery may be delayed until evacuation to echelon IV or V
2. early surgery unlikely to alter prognosis of complete spinal cord injury
3. typically performed at echelon IV/V facilities (see figure 24. C7 facet fracture with contralateral perched facet and C6 radiculopathy; figure 25. T4 fracture dislocation CT sagittal; figure 28. C7 facet fracture postoperative lateral; figure 29. T4 fracture dislocation postoperative lateral.)
{kind=link}
.jpg){kind=link}
.jpg){kind=link}
.jpg){kind=link}
4. Higher rates of neurologic improvement after surgical stabilization in patients with nonbattle injuries versus battle injuries1
5. Surgical intervention of spinal injury is associated with higher rates of complications regardless of initial injury sustained.7
References
1. Blair JA, et al. Are spine injuries sustained in battle truly different? The Spine Journal, 2011.
2. Topp, RF, Savitsky E, Cranston WP. Chapter 10: Spinal Trauma. Combat Casualty Care; Lessons Learned from OEF and OIF. 2010.
3. Schoenfeld AJ, Goodman GP, Belmont PJ. Characterization of combat-related spinal injuries sustained by a US Army Brigade Combat Team during operation Iraqi Freedom. Spine J.2010. Article in press.
4. Blair JA, et al. Military penetrating spine injuries compared with blunt. The Spine Journal, 2011.
5. Ramasamy A. Midwinter M, Majoney P, Clasper J. Learning the lessons from conflict: pre-hospital cervical spine stabilization following ballistic neck trauma. Injury. 2009;40:1342-1345.
6. Patzkowski JC, et al. Multiple associated injuries are common with spine fractures during war. The Spine Journal, 2011.
7. Possley DR, et al. Complications associated with military spine injuries. The Spine Journal, 2011.
Additional Resources
American College of Surgeons Committee on Trauma. Advanced trauma life support program for doctors, 7th ed. Chicago, IL: American College of Surgeons; 2004.
American Spinal Cord Injury Association. International standards for neurological classifications of spinal cord injury revised 2000. Chicago, IL: ASIA; 2000.
Eastridge BJ, Jenkins D, Flaherty S, Schiller H, Holcomb JB. Trauma system development in a theater of war: experiences from Operation Iraqi Freedom and Operation Enduring Freedom. J Trauma. 2006;61:1366-1373.
Teasdale JB. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81-84.
Wortmann GW, Valadka AB, Moores LE. Prevention and management of infections associated with combat-related central nervous system injuries. J Trauma. 2008;64:S252-S256.
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, Department of Defense or the U.S. Government.
Materials and support for The Disaster Preparedness Toolbox is provided by Lt Col. Ky Kobayashi, MD and Col. Benjamin Kam, MD.