

V. Axial Skeleton Injuries in an Austere Environment (continued)
CPT Jeanne Patzkowski, M.D.
CPT Chad Krueger, M.D.
B. Define the initial management, resuscitation, and stabilization of spine injuries with associated neurological injuries
Spinal Fractures with Associated Neurologic Injuries
I. Epidemiology
A. Overall spine injury from Operation Iraqi Freedom (OIF)/Operation Enduring Freedom (OEF) to date is 5.5%1
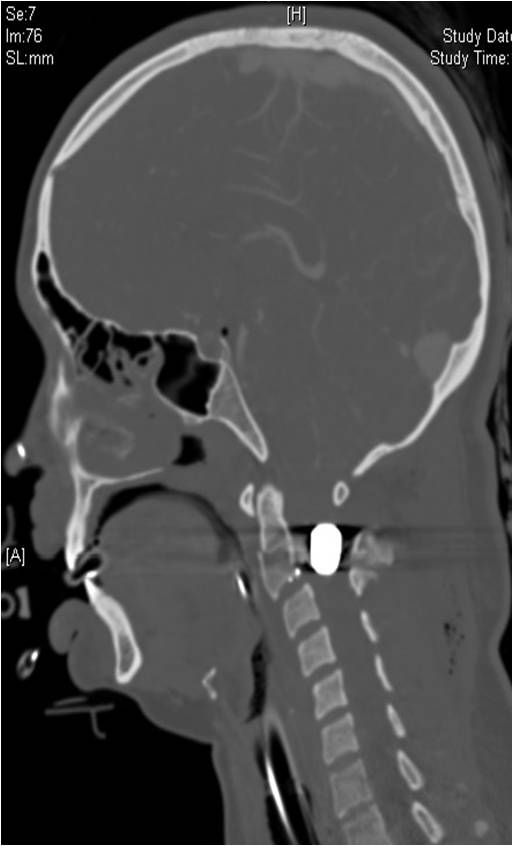
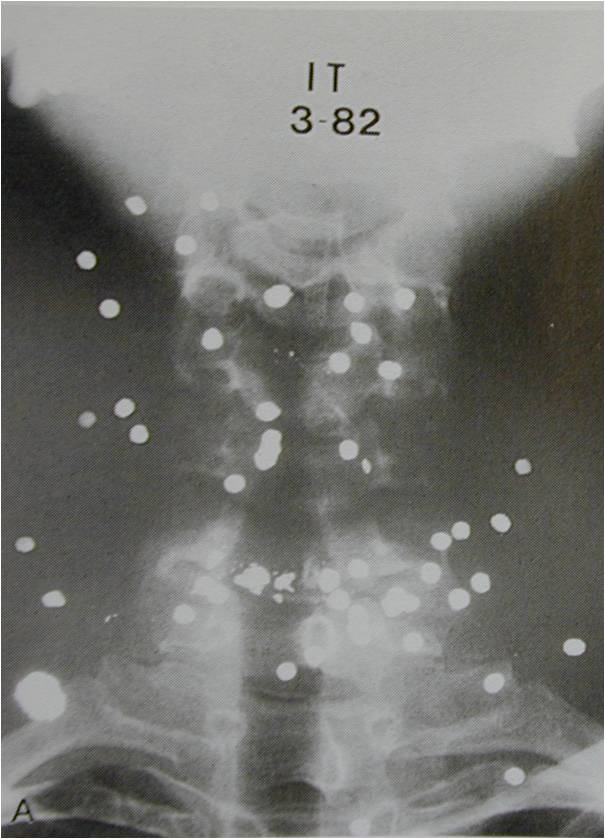
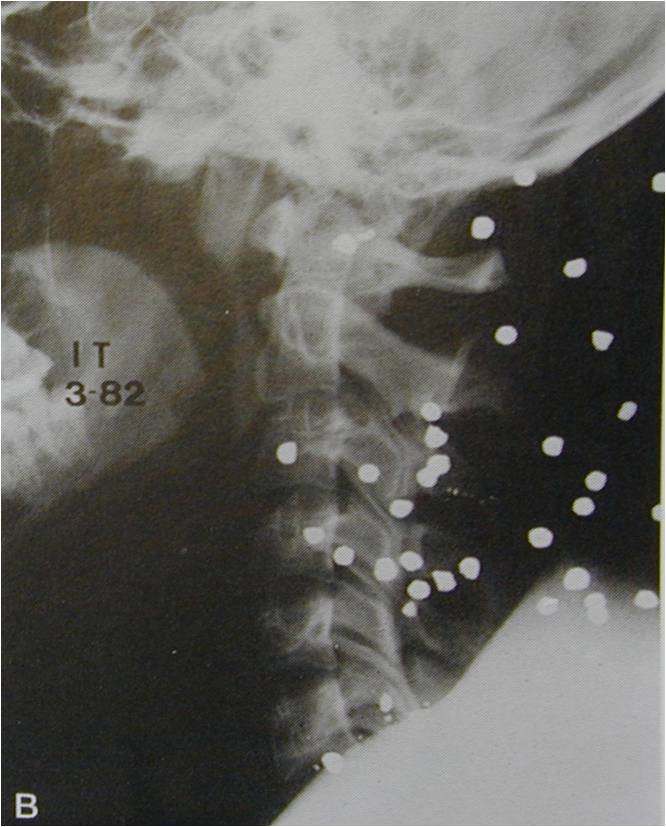
B. Increased frequency of penetrating and blast injuries in combat compared to civilian trauma2 (see figure 18. Axial CT of C2 gunshot wound; figure 19. Sagittal CT of C2 gunshot wound; figure 20. Penetrating cervical spine AP; figure 21. Penetrating cervical spine lateral.)
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
1. review of injuries sustained by Army Brigade combat team during OIF found spine injuries in 7.2% of combat casualties, 65% due to explosive mechanism; closed fractures of the spine occurred in 21%, open fractures in 7%3
2. each patient who sustained a battle spine injury sustained an average of 3.7 spine injuries. Nonbattle related injuries sustained an average of 2.8 spine injuries per patient.1
3. explosive devices accounted for 56% of all spine injuries and gunshot wounds were responsible for 15% of all spinal injuries1
4. most spine injuries occur at thoracolumbar junction
5. most common fractures
a. transverse process fractures
b. compression fractures
c. burst fractures
6. blunt trauma is likely to increase the incidence of injury to the lumbar spine when compared to penetrating trauma4
C. Risk factors for spine injury
1. spinal cord injury more common with penetrating injuries as opposed to blunt injuries4
a. bullet, fragmentation, or stab wounds near the spine
b. direct trauma to face, neck, head, or back
c. tertiary blast injury
d. major blows to head or chest
e. neurologic deficit
f. Glascow Coma Scale ≤ 8 (see figure 22. Glascow coma scale. Adapted from Teasdale, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81-84.)
.jpg){kind=link}
II. Initial Management
A. Remove wounded from hostile environment (echelon I) (may not be able to initiate spinal immobilization in zone of combat as this will endanger wounded further, along with combat casualty care provider, potentially leading to more injured soldiers
1. different from ATLS guidelines for immediate spinal immobilization once an injury above the clavicle is recognized
2. only 1.4% of Vietnam War casualties with penetrating neck trauma treated with immediate cervical spine precautions actually had a spinal injury that would have benefited from cervical spine immobilization;5 risk benefit ratio supports initiating spinal immobilization once wounded is removed to a safer location
3. most patients with normal neurological exams following penetrating neck trauma will not have a mechanically destabilized spinal column
B. Basic spinal immobilization once out of immediate danger (echelon II)
1. C-collar
2. rigid back board
C. Primary ATLS survey
1. airway, breathing, circulation, neurologic disability, exposure
2. high level cord injuries require close monitoring
a. cervical and high-thoracic injuries may affect phrenic/intercostals nerves and impair diaphragm and chest wall excursion
b. particular care must be taken with head, chest wall, and lung injuries to avoid respiratory decompensation
D. Secondary ATLS survey – thorough neurologic examination
1. there are an average of 3.5 associated injuries for patients sustaining injury to their spine in a military setting6
a. pelvis injury and TBI are common associated injuries
b. associated injuries vary dramatically depending on the mechanism of injury and level of spinal injury6
c. complete exam for awake, cooperative patients
2. if unresponsive, evaluate spontaneous movements, motor response to painful stimuli, characterization of deep tendon reflexes, rectal sphincter tone
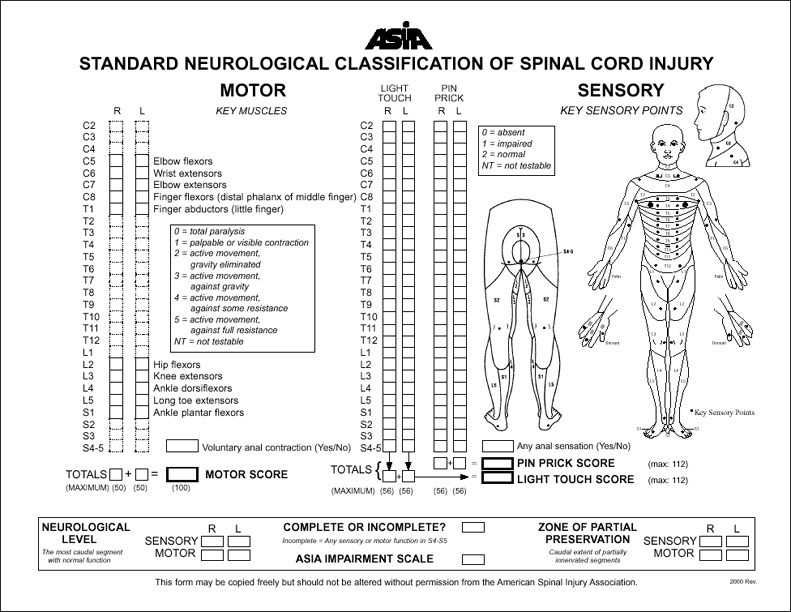
3. document exam findings and time of exam with American Spinal Injury Association (ASIA) Standard Neurological Classification of Spinal Cord Injury (see figure 23. ASIA grading scale.)
{kind=link}
4. palpate entire spinal column
a. log-roll with C-collar in proper position, maintaining in-line stabilization
b. step-off
c. inter-spinous widening
d. deformity
e. ecchymosis
f. tenderness
5. visualize wounds
a. if in proximity to known spinal injury, assume open spinal injury
b. open spinal injury defined as direct path from the skin through the dura
c. all spinal injuries associated with penetrating trauma are considered open until proven otherwise
6. motor examination
a. intact motor level is rated at ≤ 3/5 strength
c. digital rectal examination
i. voluntary sphincter contraction
ii. reflex sphincter contraction (bulbocavernosus reflex)
iii. bulbocavernosus reflex: involuntary increase in rectal tone when pressure is applied to the male glans penis or a foley catheter is tugged gently
a. light touch
b. pin-prick
c. temperature discrimination (hot vs. cold)
d. proprioception
e. full exam includes perianal region
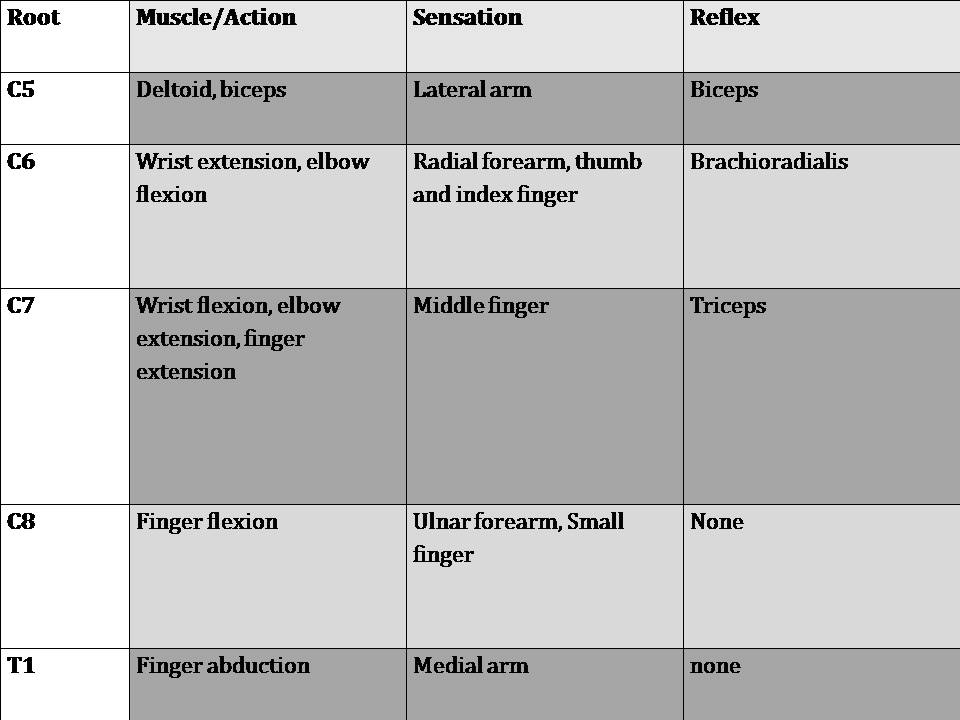
8. upper and lower extremity spinal nerves (see table 1. Upper extremity spinal nerves; table 2. Lower extremity spinal nerves. Tables adapted from Topp RF, Savitsky E, Cranston WP. Combat Casualty Care; Lessons learned from OEF and OIF, Ch. 10: Spinal Trauma, 2010.)
{kind=link}
{kind=link}
a. deep tendon reflexes
b. upper extremity spinal nerves
c. lower extremity spinal nerves
9. pathologic reflexes
a. Hoffman reflex: involuntary thumb interphalangeal joint flexion after palmar to dorsal flicking maneuver applied to middle finger distal phalanx
b. Babinski reflex: involuntary dorsiflexion of the hallux and spreading of the lesser toes in response to foreceful scratching of plantar/lateral aspect of foot
c. ankle clonus: involuntary repetitive dorsiflexion of ankle in response to one-time forceful dorsiflexion of ankle by examiner
E. Diagnostic evaluation
1. limited imaging potential at echelon II facilities
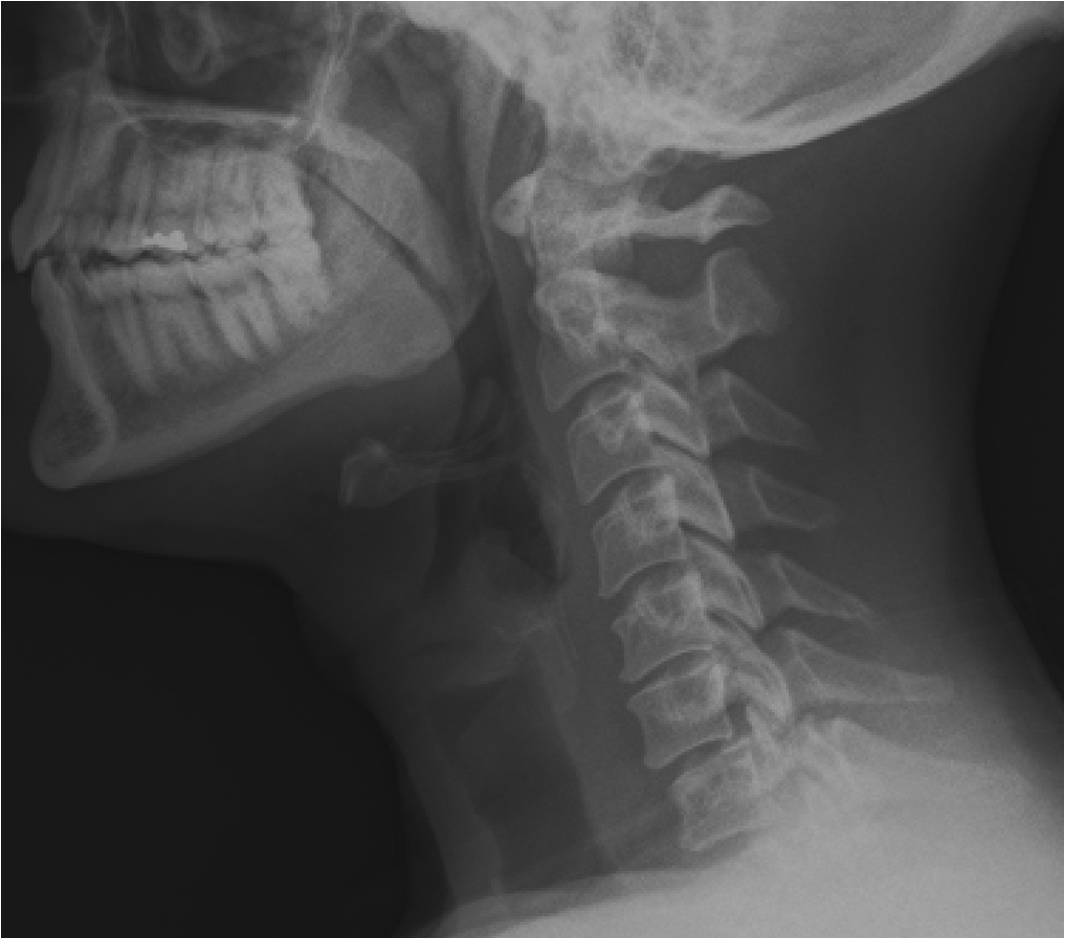
a. plain radiography (see figure 24. C7 facet fracture with contralateral perched facet and C6 radiculopathy.) – AP, lateral, odontoid views
{kind=link}
2. advanced modalities available at echelon III
a. CT scan (see figure 25. T4 fracture dislocation CT sagittal.) recommended if plain films inadequate, plain films demonstrate major fracture or dislocation, or neurologic deficit present
{kind=link}
b. laboratory support
c. blood bank
d. orthopaedic, neurosurgeon, trauma, and vascular surgeons available
e. dedicated operating rooms
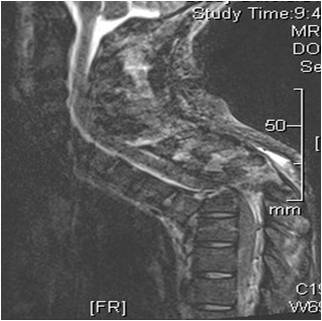
3. MRI at echelon IV and V (see figure 26. T4 fracture dislocation MRI with complete cord transaction.)
{kind=link}
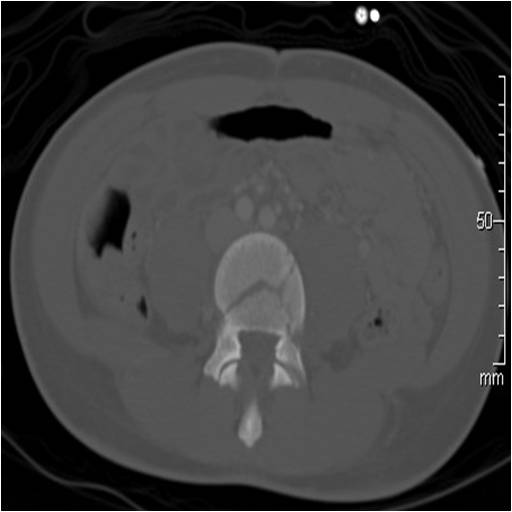
4. image and evaluate entire spine (see figure 25. T4 fracture dislocation CT sagittal; figure 27. L4 fracture associated with T4 fracture dislocation.)
.jpg){kind=link}
{kind=link}
a. 8-28% of patients with a spinal column injury will have a non-contiguous spinal injury2
b. up to 30% of these injuries are missed on initial evaluation2
III. Resuscitation
A. Airway, breathing, circulation
B. Neurogenic shock
1. flaccid paralysis with hypotension and bradycardia due to withdrawal of sympathetic tone as a result of spinal cord injury
2. treat with supportive measures: IV fluids, pressors
a. assume hypovolemia and ensure normovolemia before giving pressors
b. atropine for bradydysrhythmias
3. differentiate from spinal shock
a. a condition of abnormal neurologic function found immediately after spinal cord injury characterized by loss of spinal reflexes distal to the site of the injury
b. the end of spinal shock is heralded by return of the bulbocavernosus reflex; until the return of the bulbocavernosus reflex, the prognosis value of the motor exam is inconclusive
i. bulbocavernosus reflex: involuntary increase in rectal tone when pressure is applied to the male glans penis or a foley catheter is tugged gently
ii. bulbocavernosus reflex typically returns within 24 hours after injury
C. Avoid secondary spinal cord injury
1. hypoperfusion
a. resuscitate to ensure hemodynamic stability
b. maintain mean arterial pressure greater than 80 mmHg
2. hypoxemia
a. monitor with pulse oximetry
b. supplemental oxygen
c. keep hemoglobin levels greater than 7 g/dL
d. transfuse blood products based on clinical indications
3. mass effect – serial neurologic exams to detect evolving neurologic deficit early
D. Steroids
1. controversial for blunt trauma
2. no data to support use in penetrating trauma
3. overall not recommended in battlefield injuries
E. Prophylactic antibiotics for penetrating spinal injuries
1. no associated violation of hollow viscus
a. cefazolin, 1 g IV every 8 hours, for 3-5 days
b. if concern for meningitis, ceftriaxone 1 g IV every 12 hours
2. associated violation of hollow viscus
a. only important if viscus penetrated before projectile enters spine; if not, treat as above
b. minimal spinal debridement
c. 1-2 weeks broad-spectrum parenteral antibiotics direct against bacteria associated with the viscus in question
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, Department of Defense or the U.S. Government.
Materials and support for The Disaster Preparedness Toolbox is provided by Lt Col. Ky Kobayashi, MD and Col. Benjamin Kam, MD.