

- Discussion:
- see: elbow flexion contracture;
- indicated for patients w/ loss of motion (out of functional range from 30 to 130 deg) due to anterior and posterior osteophytes;
- PreOp Planning and Positioning:
- patient is supine w/ bump placed under shoulder, and arm folded across chest;
- equipment:
- head light is useful;
- sterile tourniquet;
- sharp small straight and curved osteotomes, sharp curved curretes, and strong pituitarys are helpful;
- bone wax;
- Operative Technique:
- standard posterior approach to elbow is performed using either triceps spliting or triceps elevating approach;
- w/ the triceps elevating technique, the ulnar nerve is identified but the cubital tunnel does not have to be released;
- the tip of the olecranon and any associated osteophytes are removed;
- take care to avoid injury to articular surface of the trochlea;
- the olecranon fossa lies just above the trochlear surface, and may contain large amounts of osteophytes;
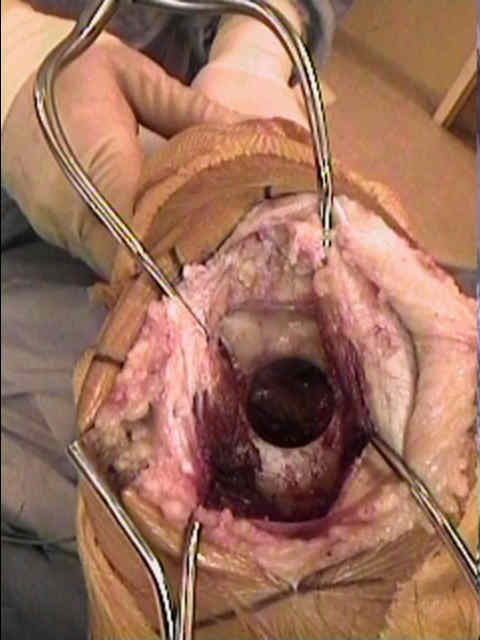
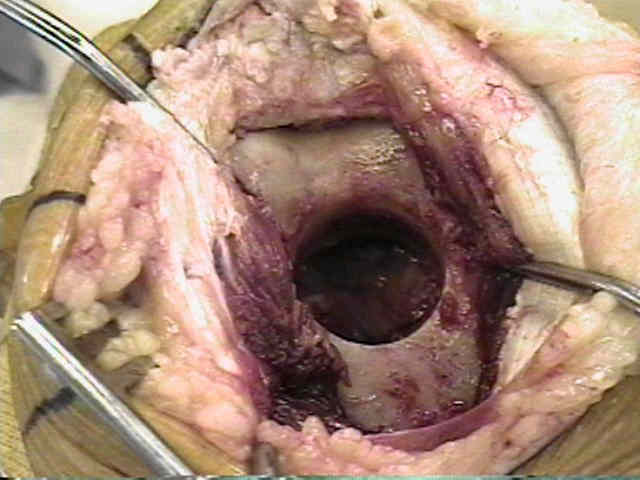
- a Cloward drill is placed in the center of the olecranon fossa and 1 sq cm of bone is removed;
- use of an excessively large Cloward drill may result in humeral fracture;
- placement of the drill hole too far inferiorly, may invade the anterior trochlear articular surface;
- some surgeons, place the drill inferiorly (just above the posterior articular surface but aim the drill slightly superiorly, in order to
avoid the anterior cartilage);
- w/ a prominent coronoid osteophyte, it is important not to place the drill hole to far superior, otherwise the surgeon will have to
currette out the osteophyte blindly ;
- elbow flexion is helpful to bring the coronoid osteophyte close to the drill hole opening;
- a currette or small osteotome is then used to remove the osteophyte;
- bone wax is applied the transected bony surfaces;
- wound closure include proximal reattachment of the triceps insertion into crossing drill holes into the olecranon, and more distally
anchoring the periosteum to the superficial forearm fascia;
- deep forearm fascia is then securely closed to prevent ulnar subluxation;
- Case Example:
- 50 year old male who developed atraumatic osteoarthritis of the elbow w/ a ROM from 40 to 120 deg;
- postoperatively, the patient had a ROM of 5 to 120 deg;


- 40 yr old male who developed atraumatic osteoarthritis of the elbow w/ a resultant ROM of 40 to 110 deg;
- post-operatively he was able to achieve 20 to 130 deg



- Complications:






Ulnohumeral Arthroplasty: Results in Primary Degenerative Arthritis of the Elbow.