

 - See:
- See: - Posterior Pelvic Injuries
- Sacral Fractures
- cresent fracture: (iliac fracture)
- Fixation Techniques:
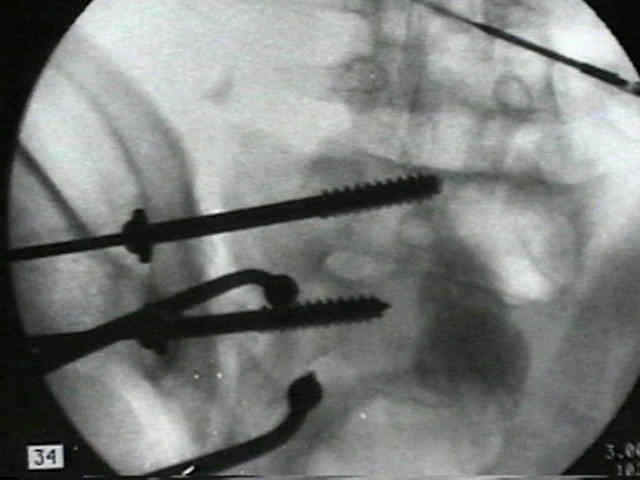
- SI joint dislocation: posterior screw fixation:
- Kellum et al 1987, unstable SI joint dislocations can produce long term pain in 60% that are treated non operatively
- associated leg length descrepancies only worse the symptoms;
- anterior fixation of SI joint dislocation:
- A Quantitative Exposure Planning Tool for Surgical Approaches to the Sacroiliac Joint.
- bilateral iliolumbar fusion
- indicated when there is bilateral unstable posterior pelvic fracture (which precludes wt bearing);
- How bilateral iliolumbar fusion increases the stability of horizontal osteosynthesis in unstable pelvic ring injuries?
------------------------------------------------------------------------------
- Older Techniques:
- transiliac sacral bars:
- utilizes Harrington rods, w/ compression achieved by tightening of threaded nuts;
- advantages include technical ease of insertion and limited soft tissue dissection;
- relative contraindications include iliac wing fractures;
- cautions: may cause over compression of sacral fractures and it can be difficult to judge adequacy of SI joint reduction;
- 4.5 mm reconstruction plate: (Albert, et al (1993));
- indicated for posterior pelvic fractures as well as sacral fractures;
- reconstruction plate is placed along dorsum of the sacral and thru the posterior iliac spines (transiliac plate fixation);
- advantages:
- low profile, minimal risk to N/V structures, and no need for flouro;
- patient is placed in the prone position;
- two incisions are made over the PSIS which are perpendicular to the iliac wings, and one vertical incision is made over the
base of the S1 spinous process;
- dissections are caarried down to the bony surfaces;
- predrill the PSIS to assist w/ reconstruction plate insertion;
- use the 4.5 drill to make 2-3 drill holes 1 cm lateral to the PSIS;
- 4.5 mm reconstruction plate is chiseled thru the iliac spine, passed along the dorsum of the sacrum to the opposite PSIS;
- the recon plate is appropriately contoured;
- the plate is fixed to the iliac wings using 6.5 mm cancellous screws, w/ two screws inserted into each ilac wing;
- postop: patients can be bed to chair or touch down wt bearing;
- ref:
- Posterior Pelvic Fixation Using a Transiliac 4.5 mm Reconstruction Plate: a clinical and biomechanical study.
- Hazards:
- wound infection and wound slough:
- especially common in posterior approaches to the joint when the pelvic frx has occured from crush injuries;
- carefully note skin abrasions, contussions, and ecchymosis over the PSIS;
- if the soft tissues are not optimal consider an anterior approach to the SI joint;
- malreduction:
- Removal of an iliosacral screw entrapping the L5 nerve root after failed posterior pelvic ring fixation: a case report.
Internal fixation of pelvic ring fractures.
Stabilization of sacroiliac joint disruption with threaded compression rods.
The crescent fracture: a posterior fracture dislocation of the sacroiliac joint.