
- Positioning and Prepping: The patient is placed on a beanbag support in the lateral position. The entire axilla to foot area is prepped with betadine solution. A waterproof stockinette is used on the lower extremity with a sterile tourniquet in place at the thigh. Betadine impregnated vidrapes are used to isolate the hip and groin as well as the leg.
- Incision:
- Deep Dissection: The vastus lateralis is then reflected to expose the lateral femur. The fascia is firmly grasped, pulled laterally, and with a knife the lateralis is removed in the avascular plane from the vastus ridge. Approximately 5 cm of lateralis is reflected. It is then tied back to the fascial edge in the inferior wound. Anteriorly, the vastus intermedialis is slowly taken down with a right angle and Stephens scissors in order to leave a trough for the ascending vessels to course in when anastamosed, so that tension is not placed on the junction. The dissection must be halted as soon as the fat layer medial to the vastus is encountered to avoid damaging the vessels. At this time a sterile draped c-arm machine is positioned over the table.
- Insertion of Guide Pin
- Bone Grafting:
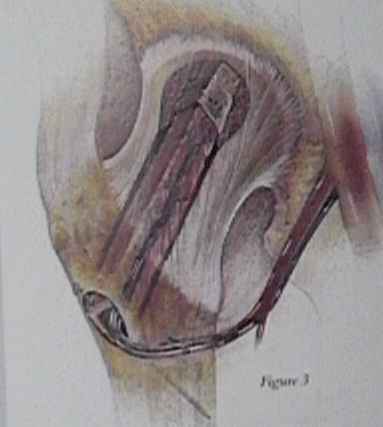
- Insertion of Fibular Graft: The renograffin must be completely removed from the cavity before placing the fibular graft. The fibula is inserted with the pedicle located at 30 degrees past vertical towards the patients head. The pedicle should be positioned into the fibular groove for better protection from the walls of the femoral tunnel. The fit should be snug but not tight. The location is checked with fluoroscope and if not seated the graft is tamped into position. A 0.62 mm wire is used to hold the graft in place. It is started on the lateral fibula and placed into the medial cortex of the lesser trochanter. Careful protection of the pedicle is carried out at this time. The fibula is held posterior to minimize any compression to the pedicle. The wire is bent over after cutting. The x-ray machine is then removed.
- Vessel Exposure:
- Wound Closure: The tensor fascia lata is not reattached during closure. The gluteal fascia is closed over a drain. If the fibula is proud in the wound the prominence can be shaved off with a high speed burr. However the pedicle is placed in danger if this is done. A running subcuticular suture is used in the skin.
